
Endocrinology — MCQs

On this page
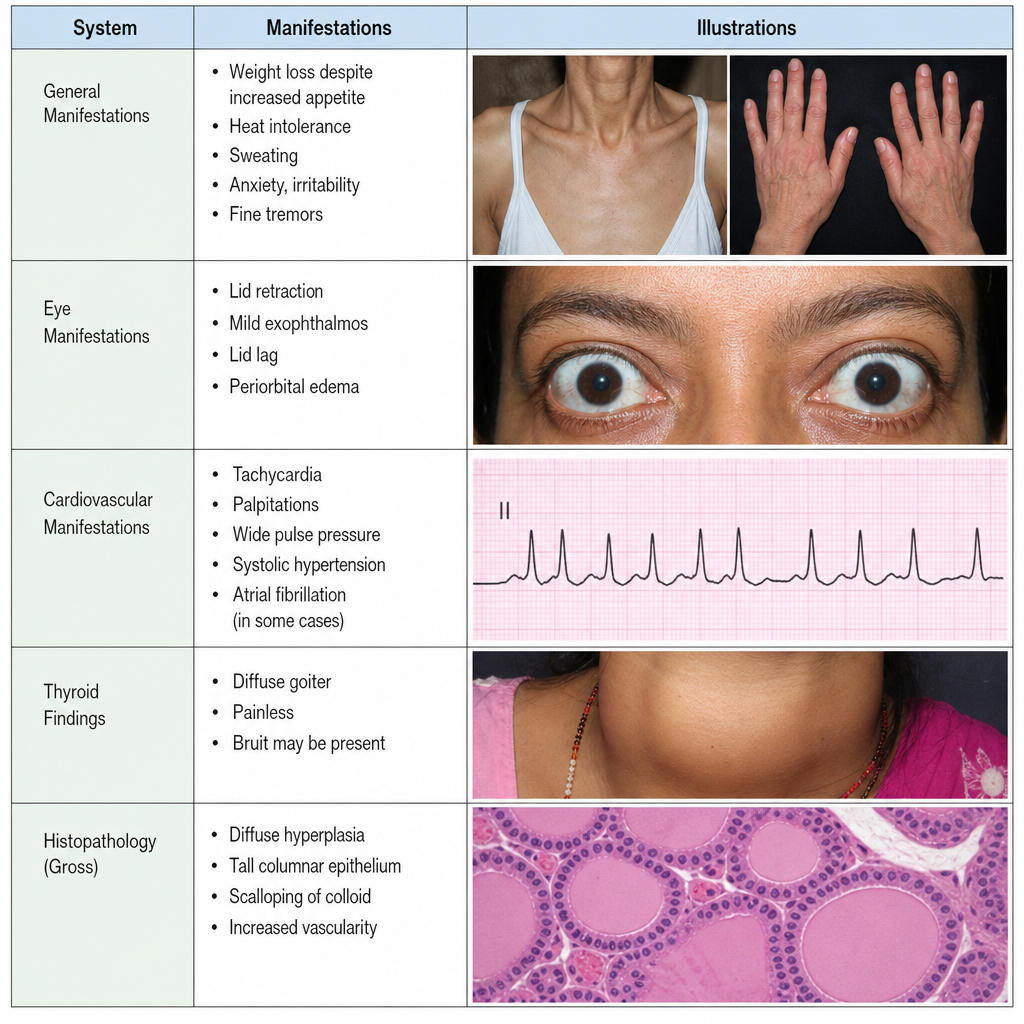
A 35-year-old woman presents with amenorrhea and weight loss despite increased appetite. The history and physical examination reveal exophthalmos, fine resting tremor, tachycardia, and warm, moist skin. What laboratory test for thyroid function would be expected to yield a decreased value?
A 30-year-old female presents with a 3-month history of 10kg weight loss despite an increased appetite. She also complains of anxiety, diarrhea, and amenorrhea. Examination reveals a fine tremor, brisk reflexes, and a systolic murmur heard throughout the precordium. A urine pregnancy screen was negative. What is the most likely finding on examining the pulse?
Which of the following findings is most consistent with the diagnosis of subacute (De Quervain's) thyroiditis?
A 53-year-old woman with metastatic breast cancer presents with lethargy, fatigue, and hypercalcemia, leading to a near-comatose state. After addressing airway, breathing, and circulation, what is the best initial therapy for this patient's hypercalcemia?
True about Chvostek's sign are all of the following except?
A 50-year-old man with a long-standing history of diabetes presents with a poor urinary stream, hesitancy, difficulty in micturition, and incomplete bladder emptying. What is the most likely diagnosis?
A 20-year-old male presents with chronic constipation, headache, characteristic habitus, neuromas of the tongue, medullated corneal nerve fibers, and a 2x2 cm nodule in the left lobe of the thyroid. What is the most likely diagnosis?
A 30-year-old pregnant woman presents for a routine physical examination. Her plasma levels of TSH are high, but her total thyroid hormone concentration is normal. Which of the following best reflects the patient's clinical state?
Which of the following statements regarding thyrotoxicosis are true? 1. Thyrotoxicosis is defined as the state of thyroid hormone excess. 2. Hyperthyroidism is a subset of thyrotoxicosis caused specifically by thyroid gland hyperactivity. 3. Thyrotoxicosis can occur without hyperthyroidism, such as in subacute thyroiditis or thyrotoxicosis factitia. 4. In Graves' disease, TSH-receptor antibodies (TRAb) stimulate the gland, leading to both hyperthyroidism and thyrotoxicosis. 5. Thyrotoxicosis and hyperthyroidism are synonymous terms, and all cases of thyrotoxicosis require antithyroid drugs (ATDs) for treatment.
Which of the following findings is NOT typically associated with hyperparathyroidism?
Practice by Chapter
Diabetes Mellitus
Practice Questions
Thyroid Disorders
Practice Questions
Adrenal Gland Disorders
Practice Questions
Pituitary Disorders
Practice Questions
Calcium and Bone Metabolism
Practice Questions
Reproductive Endocrinology
Practice Questions
Lipid Disorders
Practice Questions
Endocrine Hypertension
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Neuroendocrine Tumors
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app