
Injuries and Their Significance — MCQs

On this page
Retraction balls' after trauma are seen in which organ?
In a firearm entry wound, what is the arrangement of abrasion collar,".di" collar, and tattooing from inside to outside?
The length of a stab wound provides information about which characteristic of the weapon?
Which of the following injuries is considered a "grievous hurt"?
What is the type of fracture typically seen in battered baby syndrome?
Choking is associated with which of the following firearms?
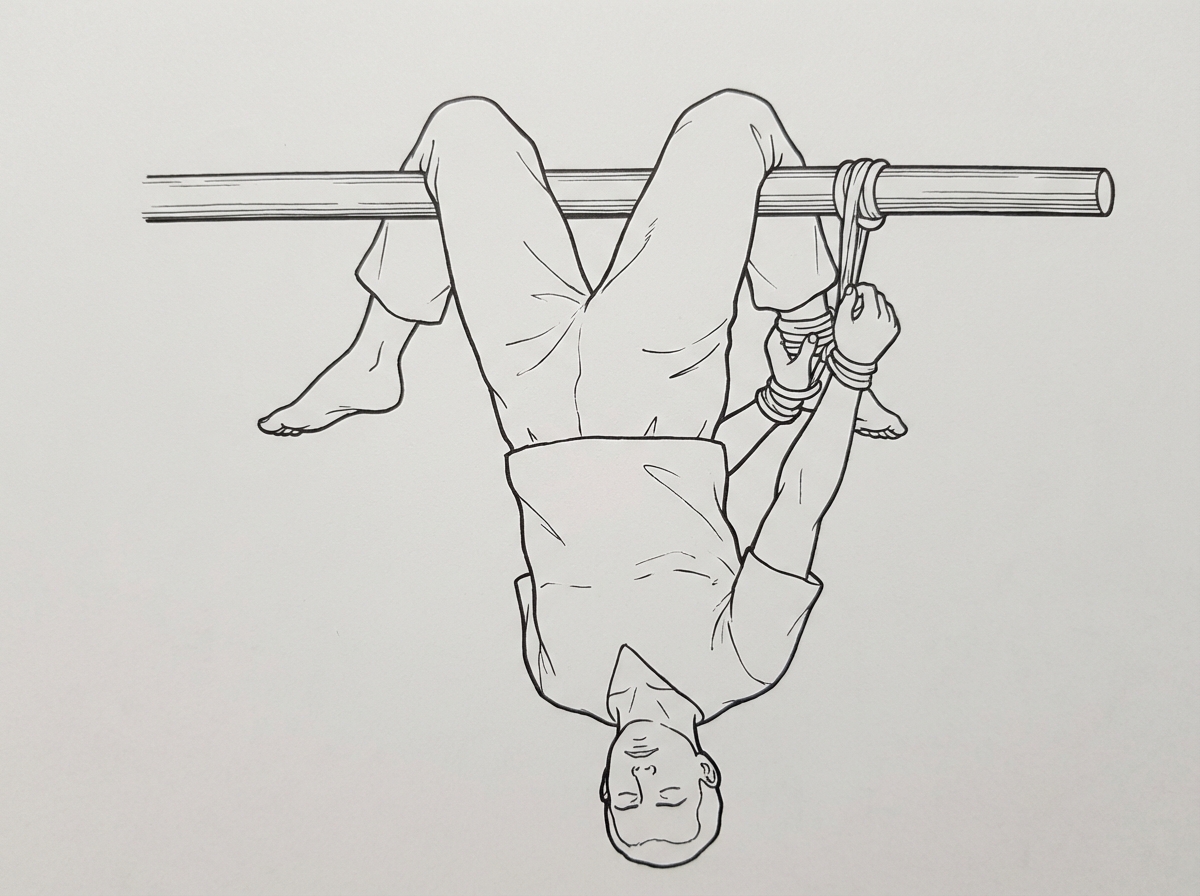
What is the name given for the torture method shown below?
Harakiri is death by:
In case of a bullet wound from a revolver, what is the indicated range when singeing of hair and charring of skin are present?
What is a characteristic difference observed in antemortem burn vesicles compared to postmortem burn vesicles?
Practice by Chapter
Mechanical Injuries
Practice Questions
Transportation Injuries
Practice Questions
Fall from Height
Practice Questions
Blunt Force Trauma
Practice Questions
Sharp Force Trauma
Practice Questions
Ballistic Injuries
Practice Questions
Burn Injuries
Practice Questions
Drowning
Practice Questions
Electrocution
Practice Questions
Lightning Injuries
Practice Questions
Explosion Injuries
Practice Questions
Pattern Injuries and Their Recognition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app