
Injuries and Their Significance — MCQs

On this page
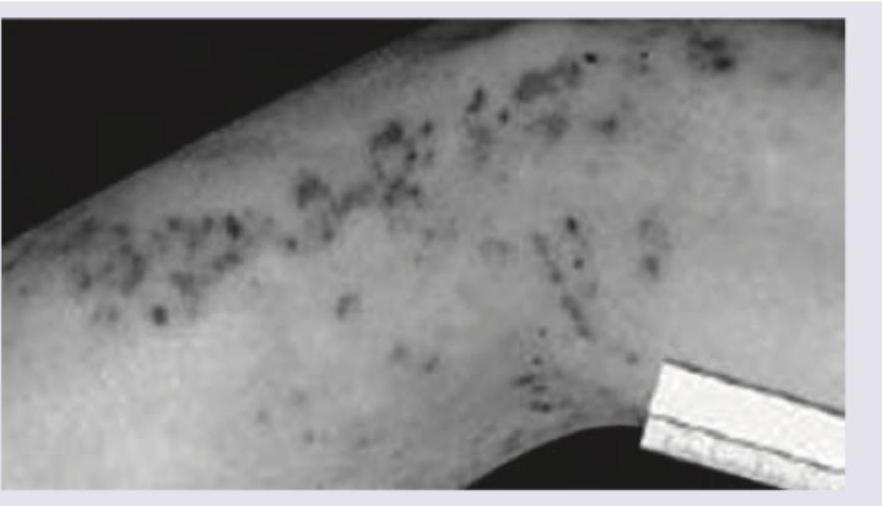
The following phenomenon is noticed in lightning strike victims. Within approximately what period do Lichtenberg figures usually fade, keeping in mind that resolution time can vary?

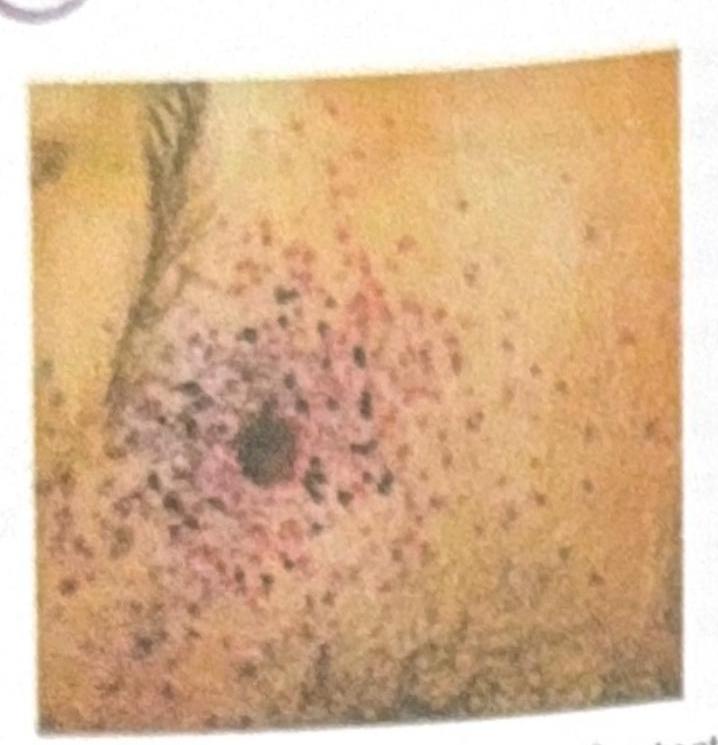
The following appearance of skin is seen in case of:
Identify the fracture given in the image given below:

The following image shows: (AIIMS Nov 2018)

Based on the image provided, identify the range of fire.
Identify the specific neck lesion shown in the image below.

Post-mortem examination of a patient reveals the following. What is this finding known as?

Match the following weapons with their corresponding injury types: Weapons: A. Axe B. RTA (Road Traffic Accident) C. Blade D. Lathi Injury Types: 5. Incised wound 6. Tram track bruise 7. Grazed abrasion 8. Chop wound
During the examination of a gunshot wound, the forensic pathologist notes an entrance wound with abrasion collar and soot deposition. The wound shows a stellate-shaped pattern with irregular margins. This pattern most likely indicates which of the following?
A 3-year-old child is brought to the emergency department with multiple bruises in various stages of healing. X-rays reveal several metaphyseal fractures and posterior rib fractures. The parents claim the injuries resulted from normal play activities. Which of the following patterns would most strongly suggest non-accidental trauma?
Practice by Chapter
Mechanical Injuries
Practice Questions
Transportation Injuries
Practice Questions
Fall from Height
Practice Questions
Blunt Force Trauma
Practice Questions
Sharp Force Trauma
Practice Questions
Ballistic Injuries
Practice Questions
Burn Injuries
Practice Questions
Drowning
Practice Questions
Electrocution
Practice Questions
Lightning Injuries
Practice Questions
Explosion Injuries
Practice Questions
Pattern Injuries and Their Recognition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app