
Injuries and Their Significance — MCQs

On this page
Identify the fracture:
What type of fracture is caused by a hammer?
A person got stabbed in his anterior thigh and died. His body was brought for postmortem. What type of injury is this?
During measurement of a rifled barrel weapon, the caliber depends on?
The triad of abrasions, bruises and punctate lacerations are typically seen in:
As per Bharatiya Nyaya Sanhita (BNS), which of the following is not classified as grievous hurt?
Identify the seeds shown below that produce artificial bruises with their juice? (Recent NEET Pattern 2016-17)

The following injury is caused due to:

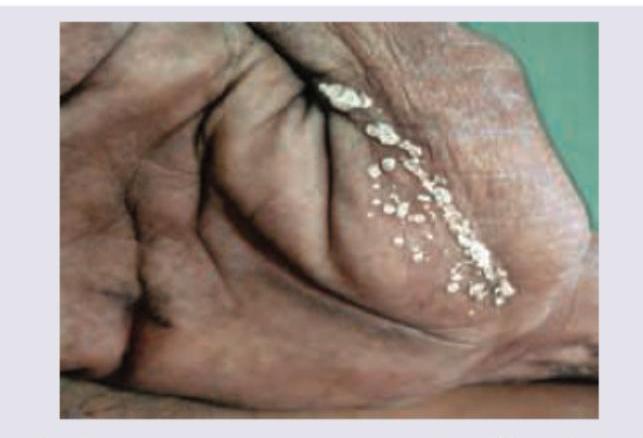
A 25-year-old person was repairing the power plug of a geyser at home when he was electrocuted and died. The image shows:

An electrician was repairing the main power line in the rainy season when he got electrocuted and died. The image of hand shows:
Practice by Chapter
Mechanical Injuries
Practice Questions
Transportation Injuries
Practice Questions
Fall from Height
Practice Questions
Blunt Force Trauma
Practice Questions
Sharp Force Trauma
Practice Questions
Ballistic Injuries
Practice Questions
Burn Injuries
Practice Questions
Drowning
Practice Questions
Electrocution
Practice Questions
Lightning Injuries
Practice Questions
Explosion Injuries
Practice Questions
Pattern Injuries and Their Recognition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app