
Injuries and Their Significance — MCQs

On this page
Comment on the range of the entry wound? (Classification used: Contact < Close range [soot + tattooing, <~30 cm] < Near range [tattooing only, ~30–60 cm] < Distant [no residue, >~60–100 cm]; all distances are approximate and firearm/ammunition-dependent.)

Ladder tears are characteristic of injuries to which vascular structure?
What is the common name for a spider web fracture?
Which of the following is FALSE about a lacerated wound?
Which part of a firearm is not a part of its gas-operating system?
What is Pupped's rule?
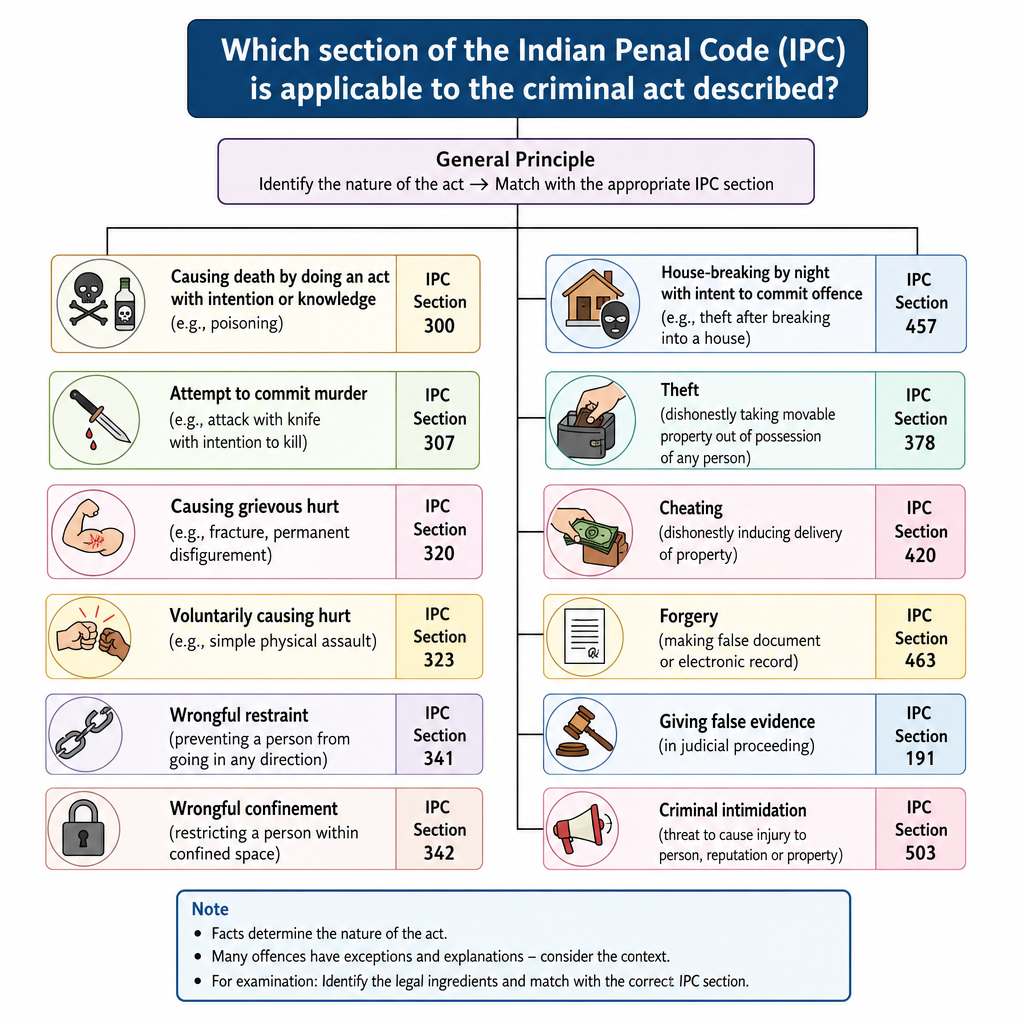
A 25-year-old woman was attacked when acid was thrown on her face, resulting in severe burns, disfigurement, and permanent disability. Which section of the Indian Penal Code (IPC) is applicable to the criminal act described?
A 26-year-old electrician is found unconscious in his backyard beside a metal ladder and an exposed electrical wire, suffering from a deep burn on his right hand. Resuscitation attempts are unsuccessful. Which of the following was the most likely cause of death?
Fg, FFg, and FFFg are terms used to describe which of the following?
Which of the following can be seen in both antemortem and postmortem burns?
Practice by Chapter
Mechanical Injuries
Practice Questions
Transportation Injuries
Practice Questions
Fall from Height
Practice Questions
Blunt Force Trauma
Practice Questions
Sharp Force Trauma
Practice Questions
Ballistic Injuries
Practice Questions
Burn Injuries
Practice Questions
Drowning
Practice Questions
Electrocution
Practice Questions
Lightning Injuries
Practice Questions
Explosion Injuries
Practice Questions
Pattern Injuries and Their Recognition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app