
Injuries and Their Significance — MCQs

On this page
What does the notation FG, FFG, FFFG indicate?
Blackening around the entry wound of a firearm injury is due to?
A patient presents with multiple injuries, including stab wounds exhibiting 'fish-tailing'. This appearance of the wound is characteristic of injury caused by:
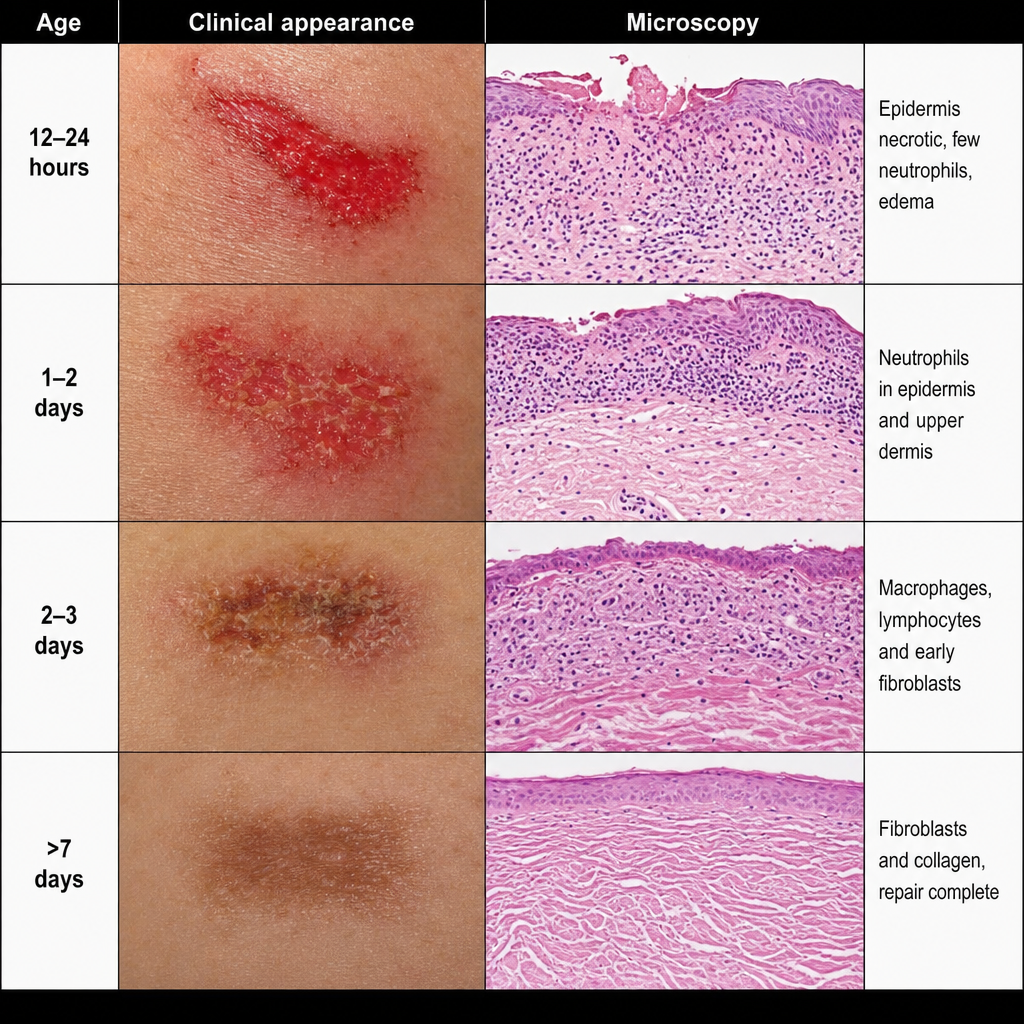
What is the age of abrasion?
The barrel of a firearm is scored internally with a number of shallow spiral grooves, called what?
In which type of injuries, contrecoup lesions are observed?
Brush burn is a type of:
Which of the following is NOT a feature of a gunshot exit wound?
Which of the following is suggestive of non-accidental injury in the pediatric age group?
In deep incised wounds, what do Langer's lines determine?
Practice by Chapter
Mechanical Injuries
Practice Questions
Transportation Injuries
Practice Questions
Fall from Height
Practice Questions
Blunt Force Trauma
Practice Questions
Sharp Force Trauma
Practice Questions
Ballistic Injuries
Practice Questions
Burn Injuries
Practice Questions
Drowning
Practice Questions
Electrocution
Practice Questions
Lightning Injuries
Practice Questions
Explosion Injuries
Practice Questions
Pattern Injuries and Their Recognition
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app