
Forensic Toxicology — MCQs

On this page
Identify the flowers shown below:

The following presentation occurs due to? (AIIMS Nov 2018)

A 40-year-old farmer attempted suicide by ingesting two aluminium phosphide (“Sulphas”) tablets. On admission, his pulse is 110 bpm, BP is 80/60 mm Hg, GCS is 7/15, and SpO2 on room air is 80%. The lead II rhythm strip shown was recorded. Which statement is false?

A child was bitten by this snake while playing. He develops blurred vision and develops hypotension with respiratory difficulty. On examination two fang marks are seen on his left foot. All are true about the management except: (Recent NEET Pattem 2016-17)
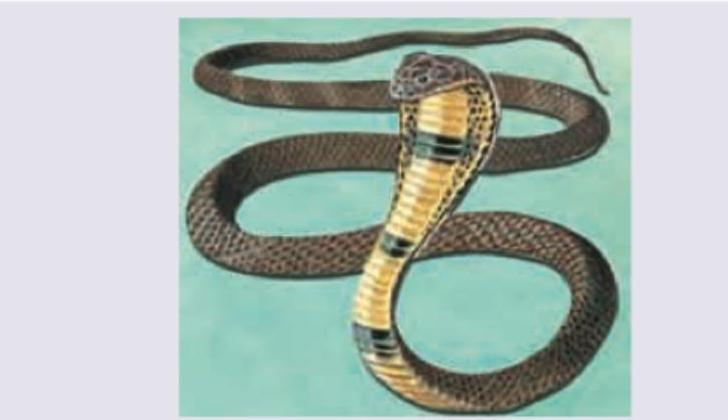
A snake charmer was bitten by a snake in the evening hours while catching a snake which had entered in the bathroom of the village sarpanch. He was brought to the hospital late at night with inability to talk and breathing difficulty. On examination gag reflex was absent, neck floppiness and tongue flaccidity was noted. His wife identified the snake from the pictures shown by the doctor as the one shown below. Which of the following should not be done in this case? (Recent NEET Pattem 2016-17)

The seeds of this plant produce which toxin?

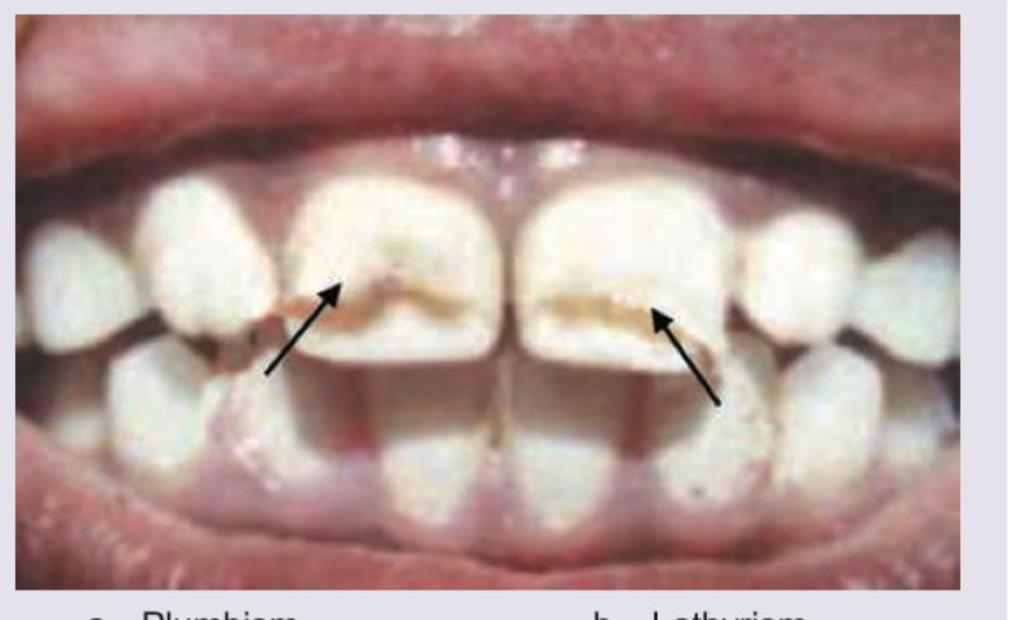
Comment on the diagnosis:
A radiopaque density may be noticed in poisoning by which of the following agents?
Which one of the following prevents gastrointestinal absorption of thallium?
Which one of the following is the correct description of Mee's lines, seen in chronic arsenic poisoning?
Practice by Chapter
General Principles of Toxicology
Practice Questions
Corrosive Poisons
Practice Questions
Metallic Poisons
Practice Questions
Non-Metallic Poisons
Practice Questions
Organic Irritant Poisons
Practice Questions
Neurotic Poisons
Practice Questions
Cardiac Poisons
Practice Questions
Asphyxiant Poisons
Practice Questions
Food Poisoning
Practice Questions
Drug Abuse and Dependence
Practice Questions
Analytical Toxicology Methods
Practice Questions
Interpretation of Toxicology Results
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app