
Forensic Toxicology — MCQs

On this page
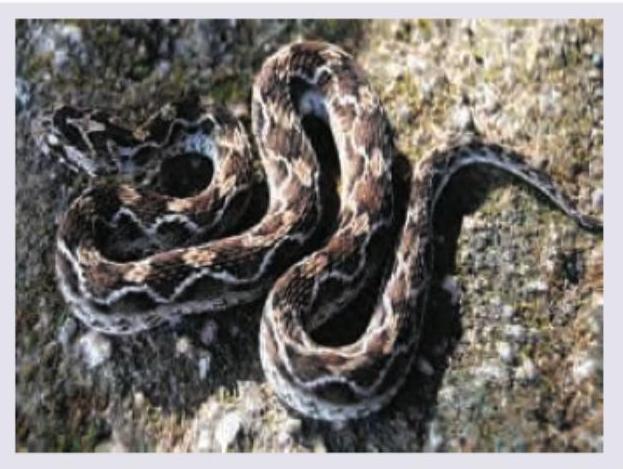
What is the type of venom of the snake shown below? (Recent NEET Pattern 2016-17)
Which snake is shown below?
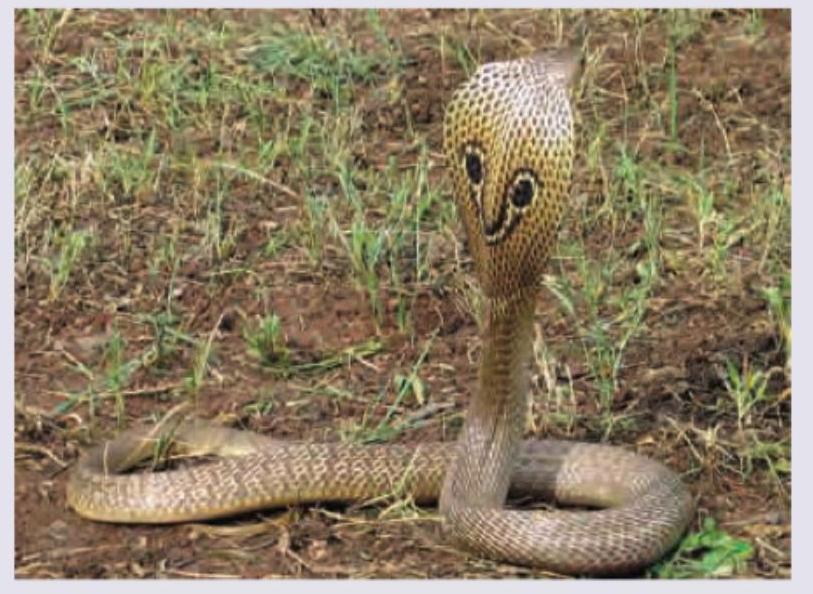
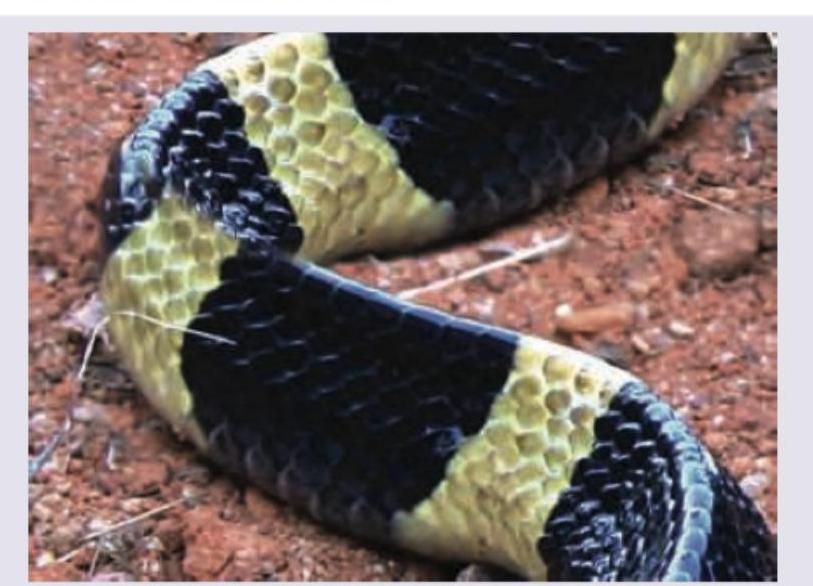
What is the nature of the venom produced by the snake shown below? (Recent NEET Pattern 2016-17)
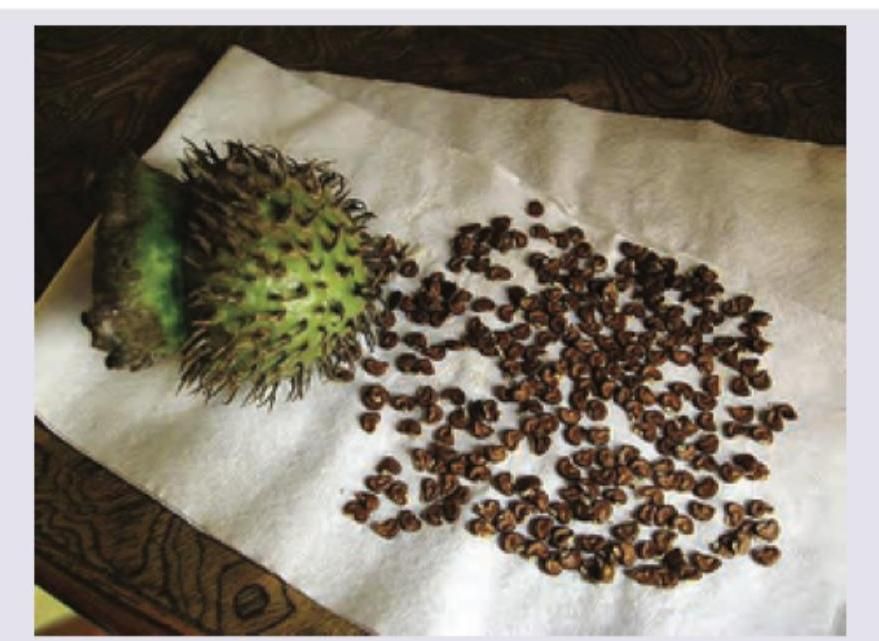
Which of the following is not true about the poisoning caused by seeds shown below?

Which of the following is not true about the symptoms experienced after consumption of the poison from the plant shown below?

The seeds of the plant shown below resemble which of the following? (Recent NEET Pattern 2016-17)
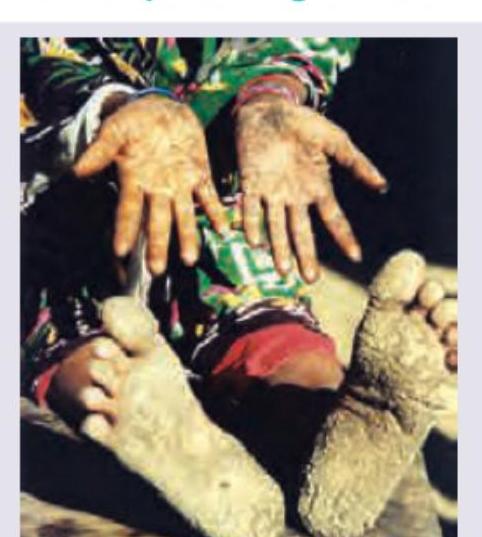
Which of the following poisonings will lead to the skin appearance shown below?

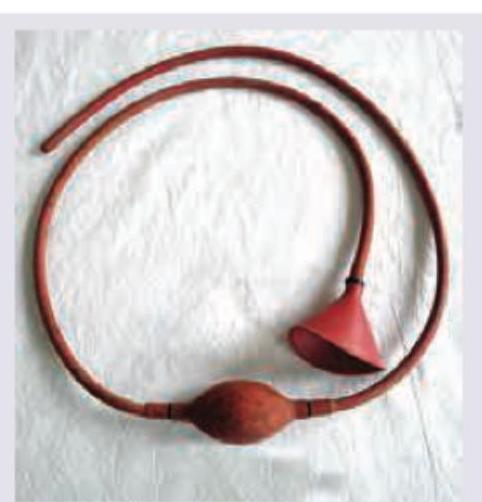
What is the function of the tube shown below?
Effects of which poisoning are shown below?
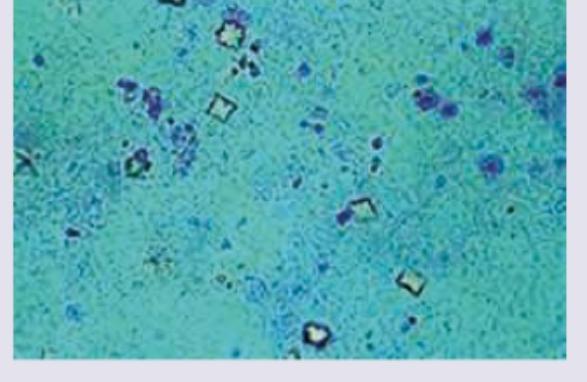
An unconscious patient was brought to the casualty. ABG reveals metabolic acidosis with hypocalcemia. The urine specimen from this patient is shown below. Identify the substance:
Practice by Chapter
General Principles of Toxicology
Practice Questions
Corrosive Poisons
Practice Questions
Metallic Poisons
Practice Questions
Non-Metallic Poisons
Practice Questions
Organic Irritant Poisons
Practice Questions
Neurotic Poisons
Practice Questions
Cardiac Poisons
Practice Questions
Asphyxiant Poisons
Practice Questions
Food Poisoning
Practice Questions
Drug Abuse and Dependence
Practice Questions
Analytical Toxicology Methods
Practice Questions
Interpretation of Toxicology Results
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app