
Forensic Toxicology — MCQs

On this page
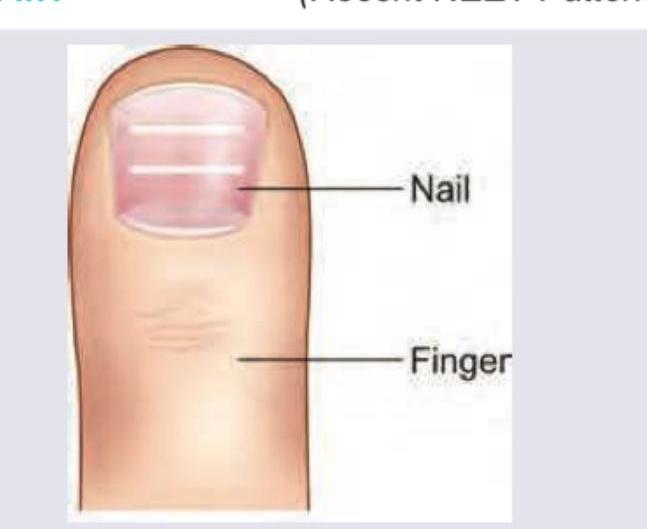
The appearance of lines in nails as shown below is classically associated with which poisoning? (Recent NEET Pattern 2016-17)
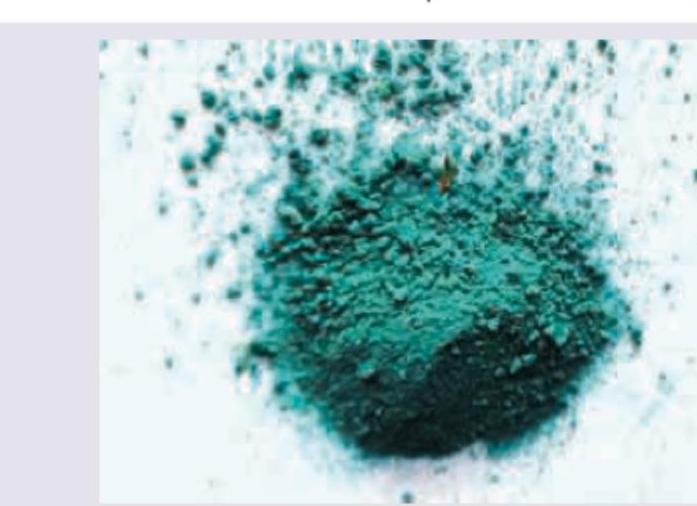
The toxin shown in the image will lead to the development of: (Recent NEET Pattern 2016-17)

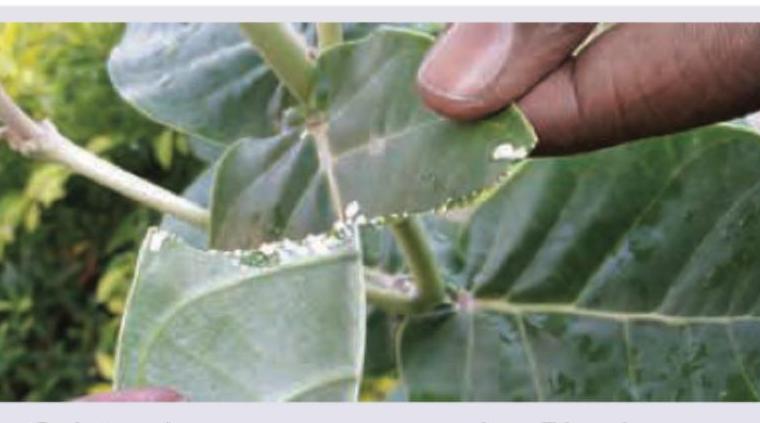
Identify the plant shown in the image:
A patient presents with lead poisoning. Which of the following hematologic findings is expected to develop?
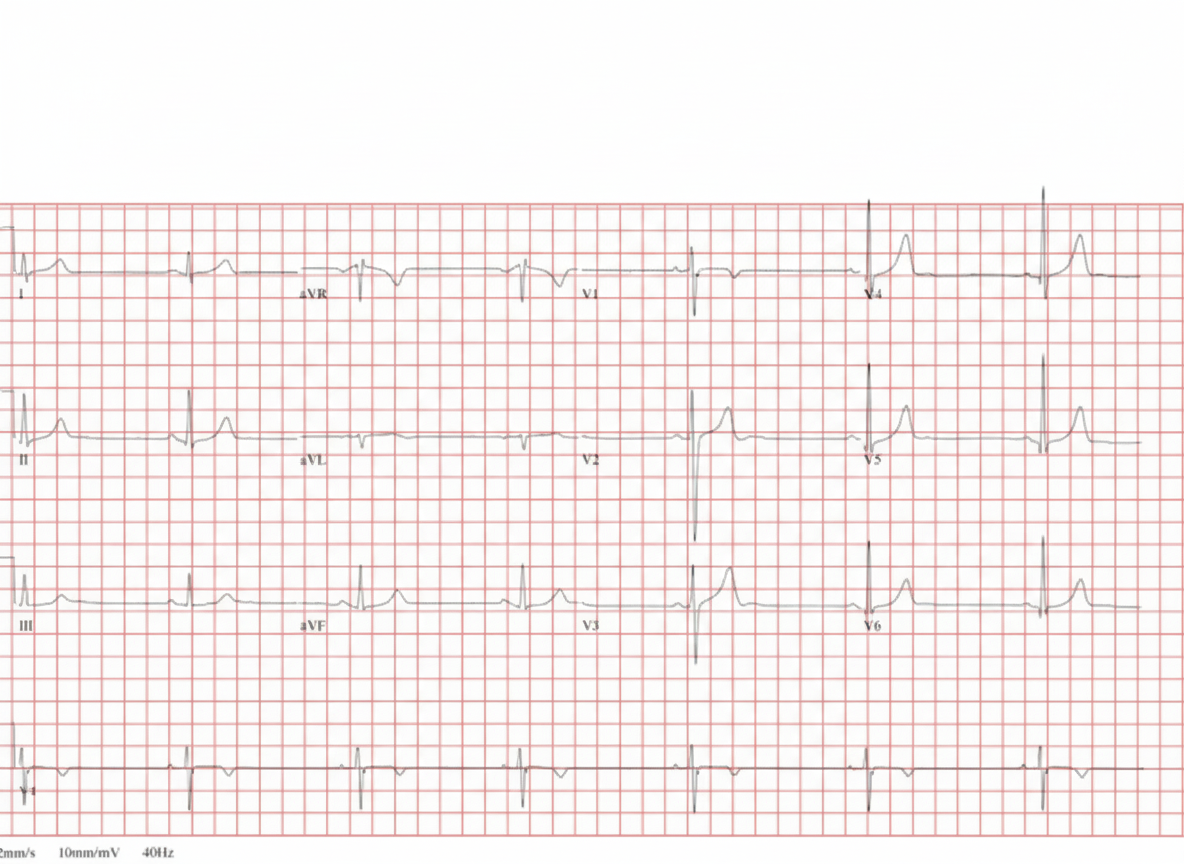
A patient from a rural tropical region presents with nausea, vomiting, and life-threatening cardiac arrhythmias after ingesting seeds from a plant found in their garden. The ECG changes are shown below. Identify the most likely toxin responsible. (Recent NEET Pattern 2016-17)
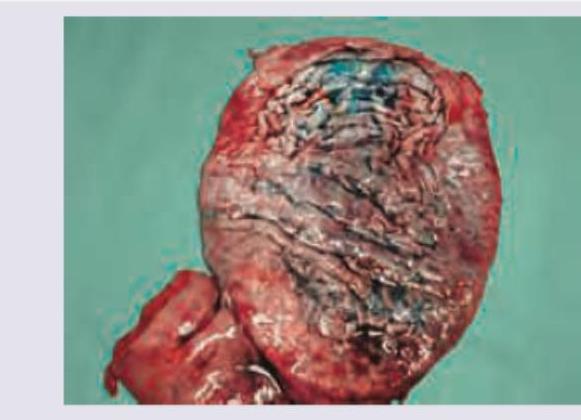
Which of the following toxins will lead to the appearance of gastric mucosa as shown in the image?
The image given below shows:
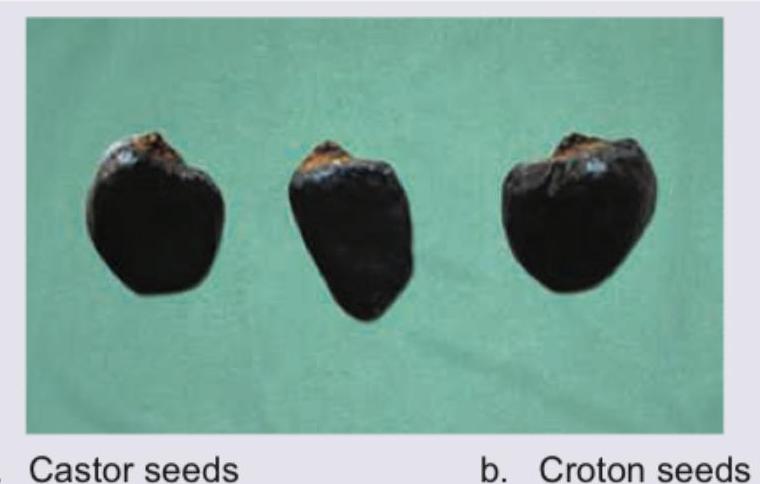
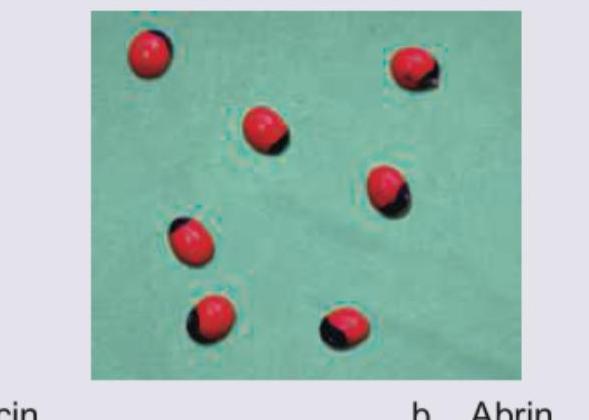
The seeds shown in the image below have which toxin? (Recent NEET Pattern 2016-17)
The following image shows:

All are true about the poisoning caused by following plant except: (Recent NEET Pattern 2016-17)

Practice by Chapter
General Principles of Toxicology
Practice Questions
Corrosive Poisons
Practice Questions
Metallic Poisons
Practice Questions
Non-Metallic Poisons
Practice Questions
Organic Irritant Poisons
Practice Questions
Neurotic Poisons
Practice Questions
Cardiac Poisons
Practice Questions
Asphyxiant Poisons
Practice Questions
Food Poisoning
Practice Questions
Drug Abuse and Dependence
Practice Questions
Analytical Toxicology Methods
Practice Questions
Interpretation of Toxicology Results
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app