
Forensic Toxicology — MCQs

On this page
What is the characteristic symptom of arsenic poisoning?
Which of the following does not refer to a cannabis preparation?
Postmortem luminescence is associated with the ingestion of which of the following substances?
An alcohol addict consumed methyl alcohol containing ethanol. All of the following are true about methanol poisoning, EXCEPT?
A family of four presents with a burning sensation over the extremities. Some members also experience vomiting, diarrhea, dilated pupils, and occasional muscle spasms. What is the MOST likely cause of these symptoms?
Which of the following toxalbumins is used as a terrorist weapon?
Golden hair is seen in poisoning with which substance?
A patient with a long history of depression on antidepressants presents with bradycardia, hypersalivation, and miosis after consuming an unknown substance. What is the most probable diagnosis?
Hemodialysis is used in the management of poisoning by all of the following agents except:
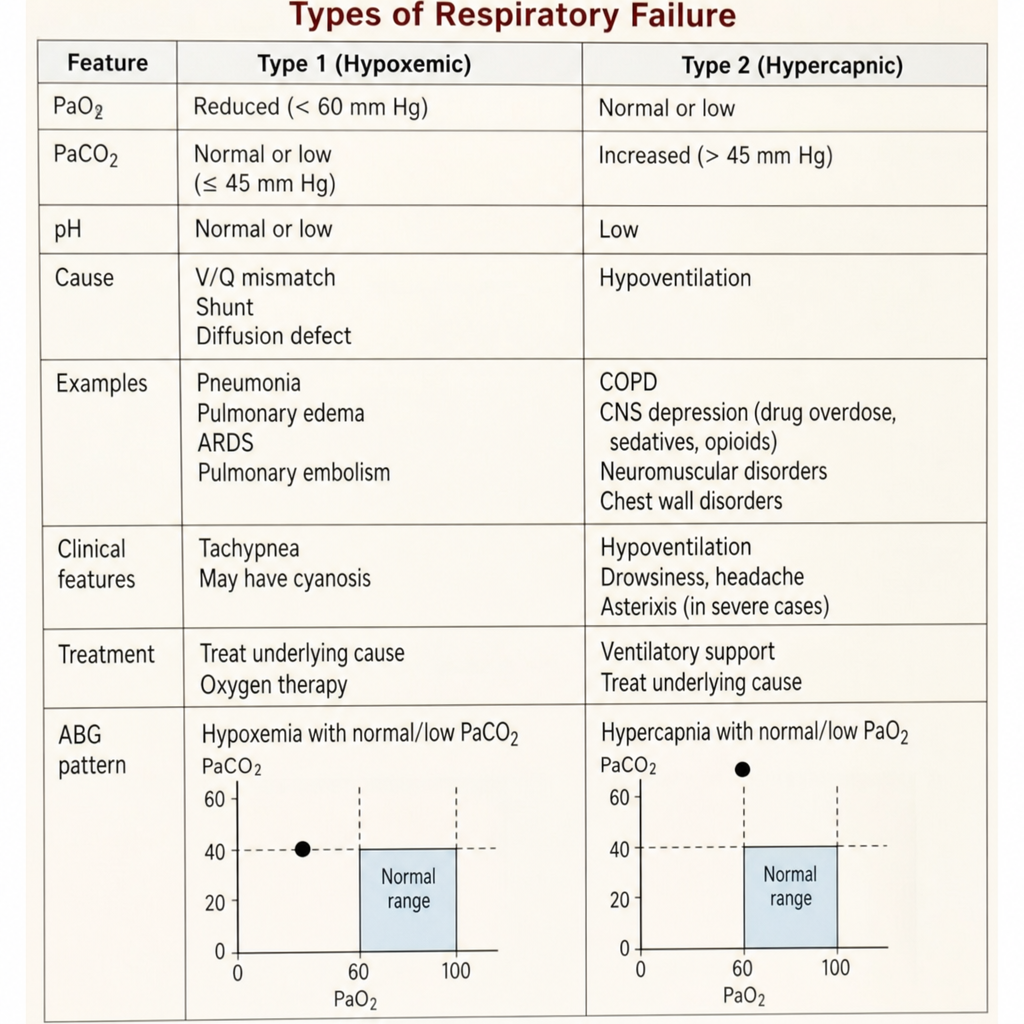
Which of the following statements regarding respiratory failure in poisoning is true?
Practice by Chapter
General Principles of Toxicology
Practice Questions
Corrosive Poisons
Practice Questions
Metallic Poisons
Practice Questions
Non-Metallic Poisons
Practice Questions
Organic Irritant Poisons
Practice Questions
Neurotic Poisons
Practice Questions
Cardiac Poisons
Practice Questions
Asphyxiant Poisons
Practice Questions
Food Poisoning
Practice Questions
Drug Abuse and Dependence
Practice Questions
Analytical Toxicology Methods
Practice Questions
Interpretation of Toxicology Results
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app