
Forensic Toxicology — MCQs

On this page
An individual with a history of alcoholism presents with poor judgment and decreased skilled motor movements. What is the expected blood alcohol level?
Organophosphorus insecticides are all, except:
Delayed rigor mortis is a characteristic finding in which type of poisoning?
A 10-year-old boy consumes stain remover and presents with 'coffee-coloured' vomiting and restlessness. What is the most likely diagnosis?
Peripheral neuritis with characteristic ‘wrist drop’ or 'foot drop' is seen in which type of poisoning?
Which of the following is FALSE about Hydrocyanic acid?
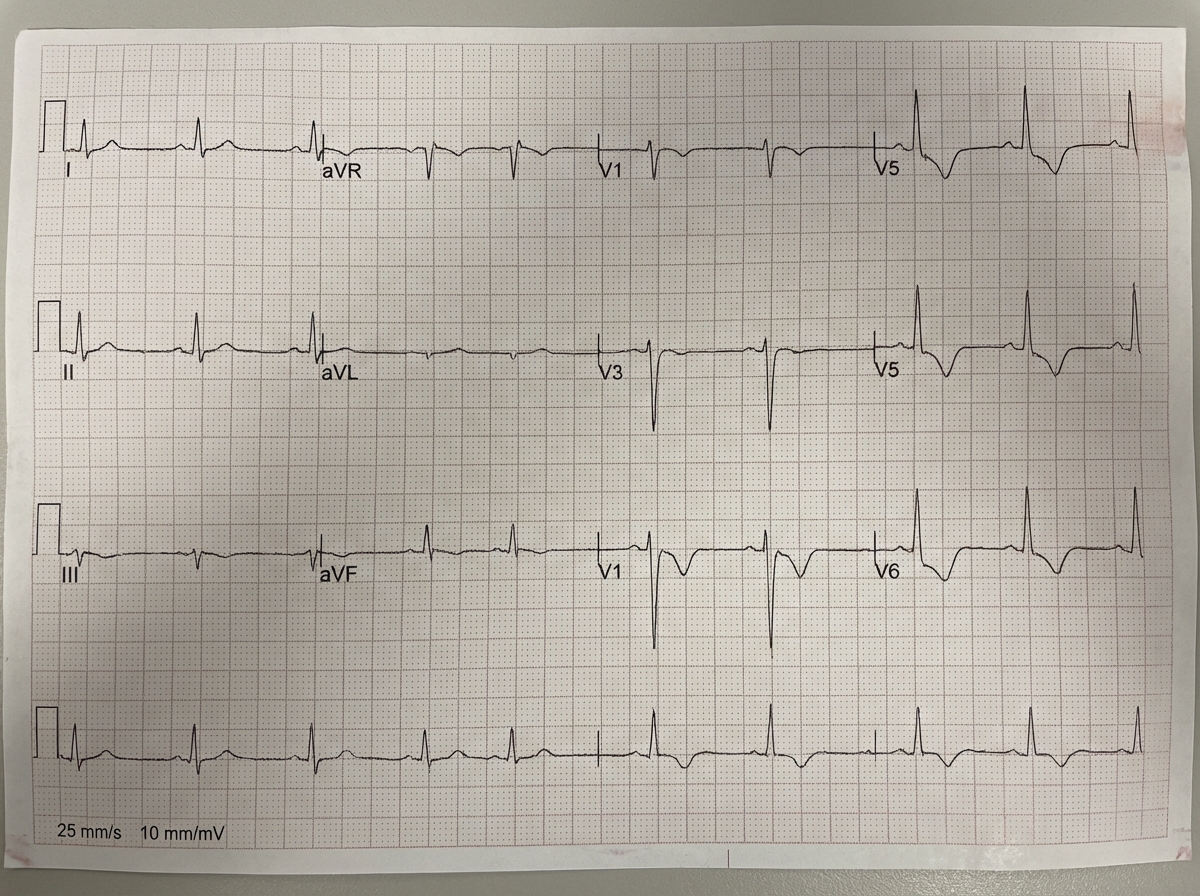
A 10-year-old girl was admitted to the emergency room with a history of ingesting 10 crushed seeds of an unknown plant. Her ECG showed specific abnormalities. What is the probable cause of these ECG changes?
Two individuals presented with symptoms and subsequently died. A distinctive smell of bitter almonds was noted emanating from their mouths. These deaths are suspected to be due to which poison?
A middle-aged man presents with paresthesia of the hands and feet. Examination reveals 'Mees' lines in the nails and raindrop pigmentation on the hands. What is the most likely causative toxin for these symptoms?
A 40-year-old man, working in a farm, presented with headache, malaise, a sense of tightness, dimness of vision, excessive salivation, and diarrhea. On examination, pupils were shown as below. What is the diagnosis?

Practice by Chapter
General Principles of Toxicology
Practice Questions
Corrosive Poisons
Practice Questions
Metallic Poisons
Practice Questions
Non-Metallic Poisons
Practice Questions
Organic Irritant Poisons
Practice Questions
Neurotic Poisons
Practice Questions
Cardiac Poisons
Practice Questions
Asphyxiant Poisons
Practice Questions
Food Poisoning
Practice Questions
Drug Abuse and Dependence
Practice Questions
Analytical Toxicology Methods
Practice Questions
Interpretation of Toxicology Results
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app