
Vestibular Disorders — MCQs

On this page
Vasodilators in Meniere's disease are useful because they:
All are features of Meniere's disease except:
In the caloric test, cold water stimulation causes movement of the eye towards which side?
A 50-year-old female complains of an episode of acute vertigo with vomiting and unsteadiness and light-headedness, which was triggered by changing her head position in the morning. She denied hearing loss, recent viral illness, medication use, head injury, or trauma. Choose the most appropriate diagnosis:
The following test is useful for diagnosis of?

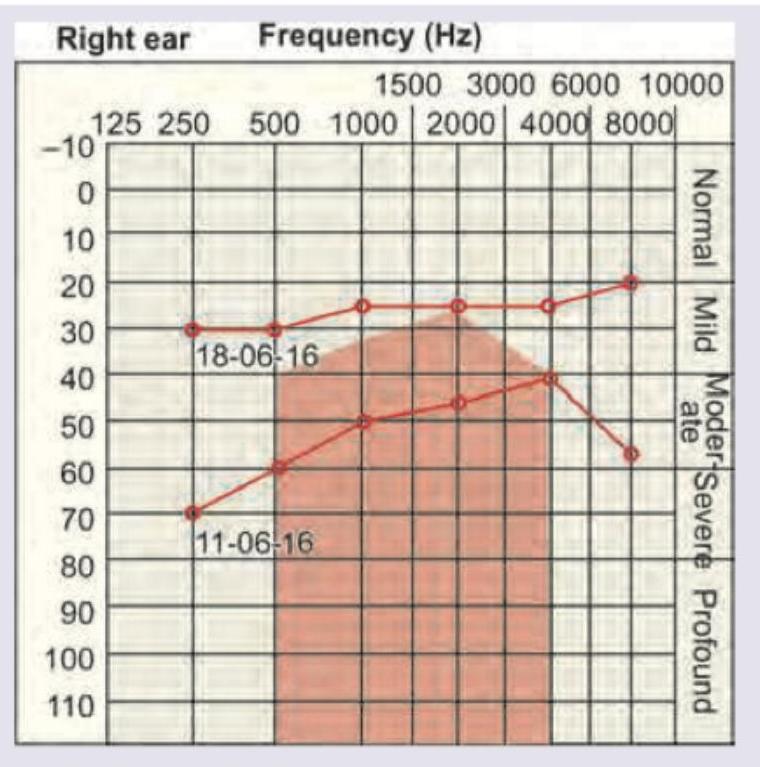
A 40-year-old woman presents with history of recurrent episodes of spinning sensation in horizontal direction with vertigo incapacitating her for hours and resolving with medication. She also report roaring tinnitus during the attacks. Her sequential audiogram done on 11.06.16 and 18.06.16 is given below. Diagnosis is:
Which of the following test is being performed on the patient?

In a patient with right vestibular neuronitis, what will be the finding on the head impulse test?
A patient presents with vertigo, tinnitus, and head tilt. He underwent myringoplasty for the safe type of chronic suppurative otitis media (CSOM) 6 months back. What is your diagnosis?
35 years old female presents with tinnitus, vertigo and aural fullness. Likely diagnosis:
Practice by Chapter
Anatomy and Physiology of Balance
Practice Questions
Vestibular Testing Methods
Practice Questions
Videonystagmography
Practice Questions
Rotational Chair Testing
Practice Questions
Vestibular Evoked Myogenic Potentials
Practice Questions
Video Head Impulse Test
Practice Questions
Benign Paroxysmal Positional Vertigo
Practice Questions
Vestibular Neuritis
Practice Questions
Ménière's Disease
Practice Questions
Vestibular Migraine
Practice Questions
Central Vertigo
Practice Questions
Vestibular Rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app