
Pediatric Otolaryngology — MCQs

On this page
Which of the following is the commonest cause of stridor in a newborn?
Which of the following is indicative of a foreign body in the tracheobronchial tree in a child?
What is the most common manifestation of HPV infection in children?
What is the narrowest part of the infantile larynx?
Which of the following syndromes is most commonly associated with clefts of the lip and palate?
What are the clinical features of submucous cleft deformity?
In a child with a suspected foreign body in the lung, what is the next best step in management?
A retroauricular incision in children less than 2 years of age may cause damage to which cranial nerve?
What is the immediate management of a child with foreign body inhalation?
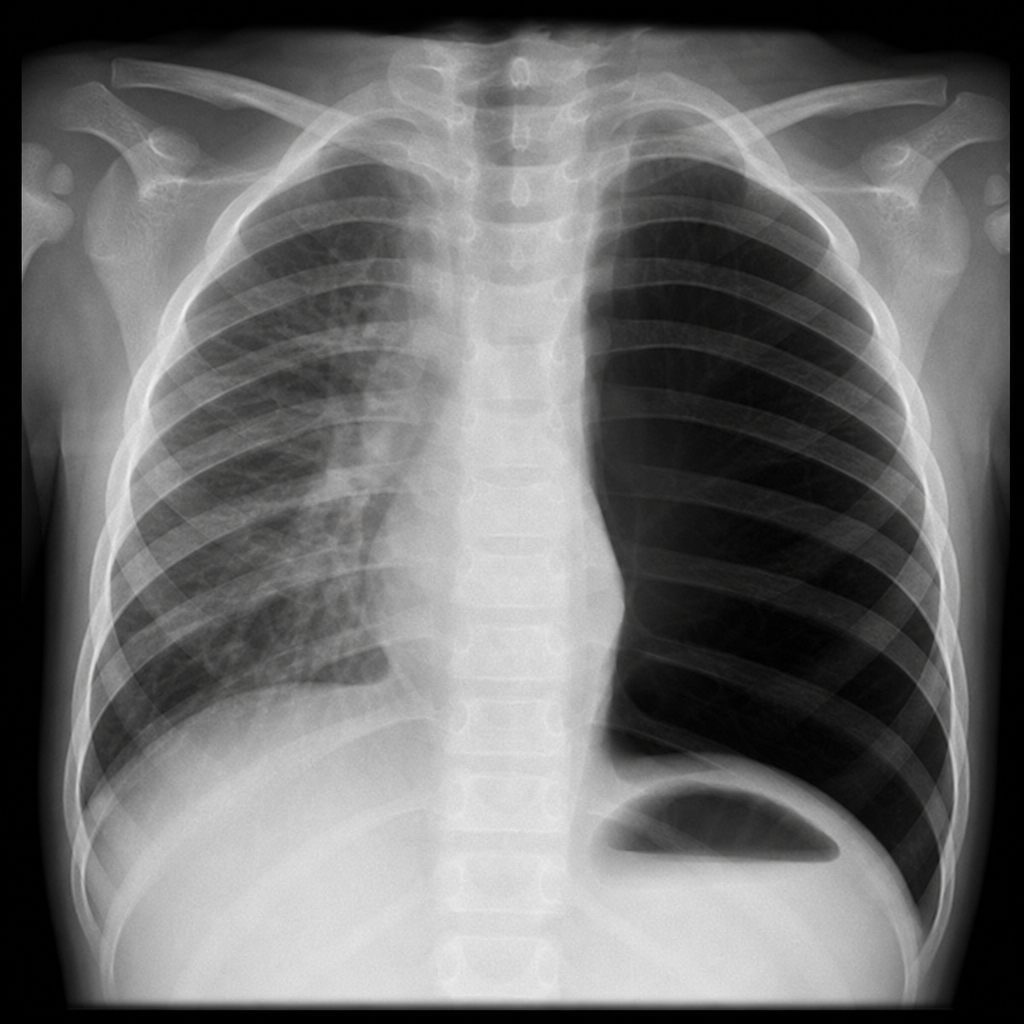
A 2-year-old child developed sudden bouts of cough, breathlessness, and respiratory distress after choking on a small radiolucent object during play. A chest X-ray was performed. What is the probable diagnosis?
Practice by Chapter
Congenital Anomalies of the Ear
Practice Questions
Pediatric Hearing Loss
Practice Questions
Otitis Media in Children
Practice Questions
Pediatric Sinusitis
Practice Questions
Pediatric Sleep Apnea
Practice Questions
Stridor in Children
Practice Questions
Congenital Airway Anomalies
Practice Questions
Foreign Body Management
Practice Questions
Pediatric Head and Neck Masses
Practice Questions
Pediatric Tracheostomy
Practice Questions
Pediatric Voice Disorders
Practice Questions
Pierre Robin Sequence and Airway Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app