
Otology — MCQs

On this page
A 9-year-old girl presents with painful swelling behind her ear. An MRI reveals mastoiditis. Which of the following structures is most likely to be affected by the inflammation?
A child presents with ear infection with foul-smelling discharge. On further exploration, a small perforation is found in the pars flaccida of the tympanic membrane. What is the most appropriate next step in management?
All of the following structures are removed during a radical mastoidectomy except?
What is the ossicular ratio?
Simple mastoidectomy is indicated for which of the following conditions?
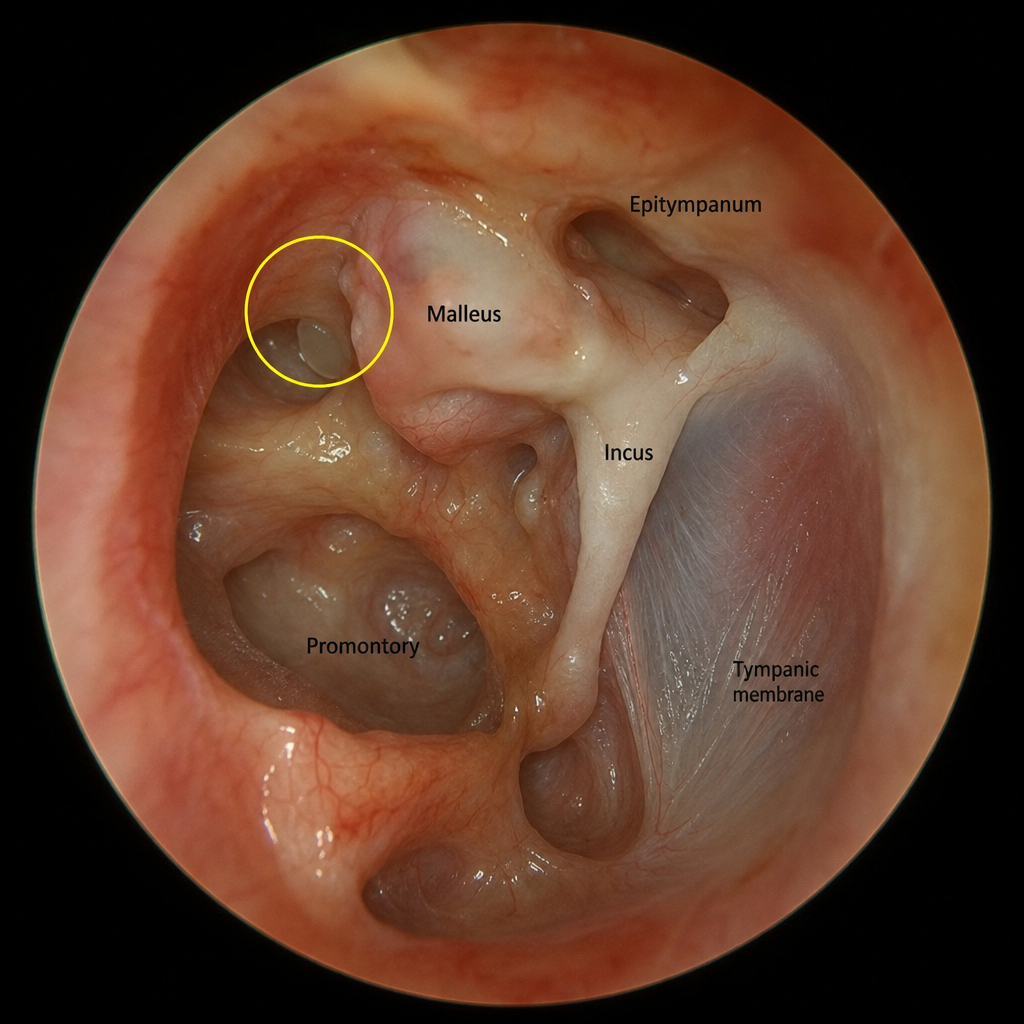
What anatomical structure is indicated by the encircled area?
All are true about otosclerosis except?
What is the resonance frequency of the tympanic membrane?
Communication between the middle ear and Eustachian tube is obliterated in which surgery?
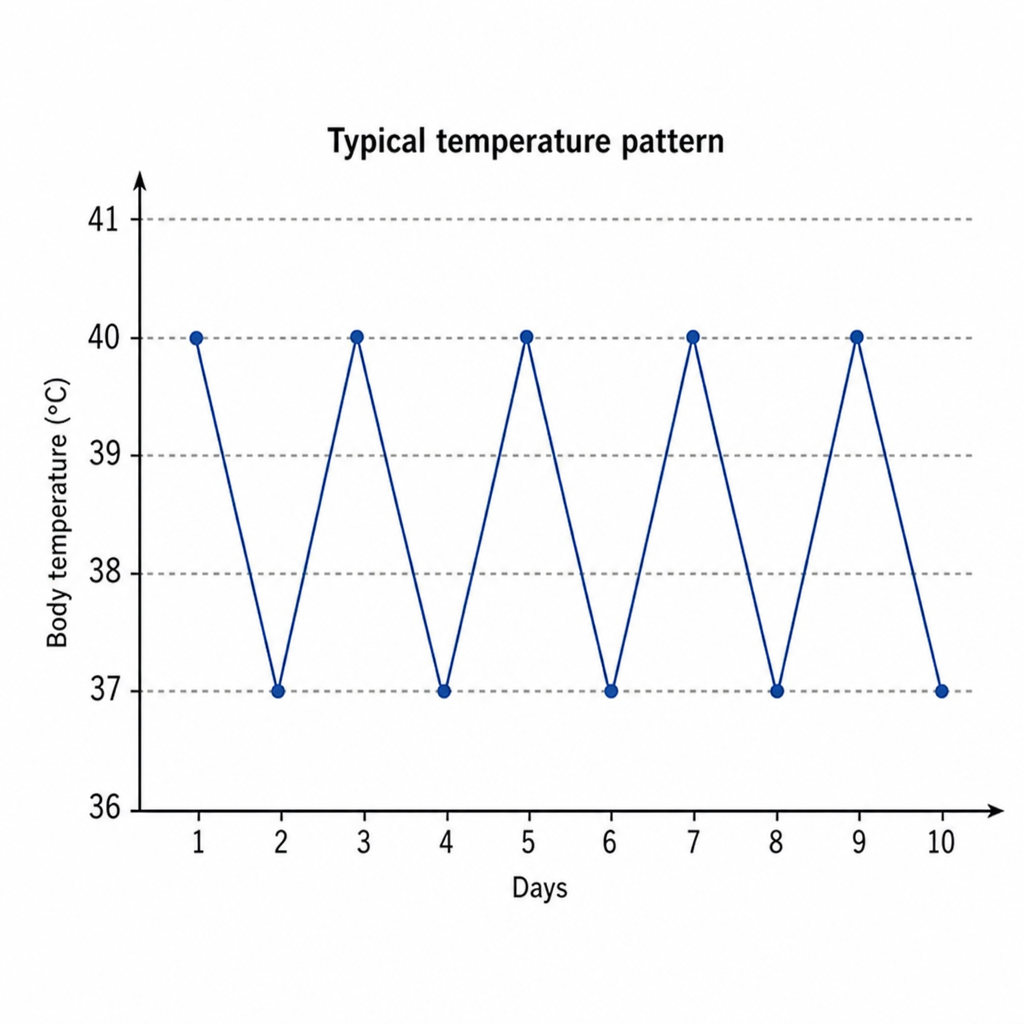
What is the characteristic temperature pattern seen in?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app