
Otology — MCQs

On this page
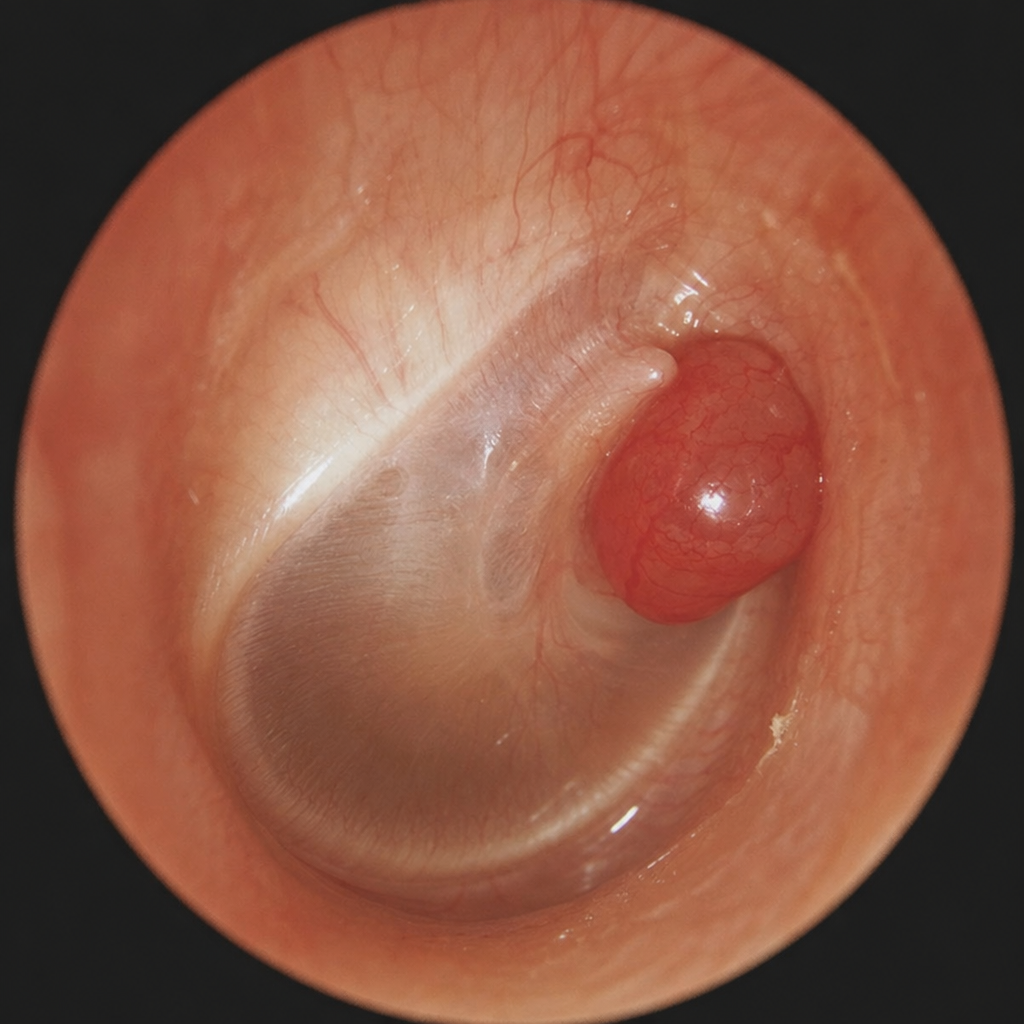
A 60-year-old lady presented with mild hearing loss and pulsatile tinnitus of the right ear. Otoscopy revealed specific findings. What is the most probable diagnosis?
In the pathogenesis of otosclerosis, where does the disease process begin?
A patient with chronic suppurative otitis media (CSOM) has cholesteatoma and presents with vertigo. What is the treatment of choice?
Gradenigo's syndrome is characterized by all except?
A patient with a history of head injury presents with unilateral conductive hearing loss. Examination reveals a normal and mobile tympanic membrane. What is the most likely cause for the deafness?
Gradenigo's syndrome is due to:
Pure-tone audiometry of a 30-year-old field worker shows Carhart's notch. What is the likely underlying condition?
Edema over the mastoid is seen in which condition?
In otosclerosis, tinnitus is most commonly due to which of the following?
What is the most common site for the initiation of otosclerosis?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app