
Otology — MCQs

On this page
Which one of the following conditions produces sensorineural deafness ?
A female patient's pure tone audiometry (PTA) findings show the presence of a Carhart's notch. Which of the following specific clinical signs can be seen in this patient?
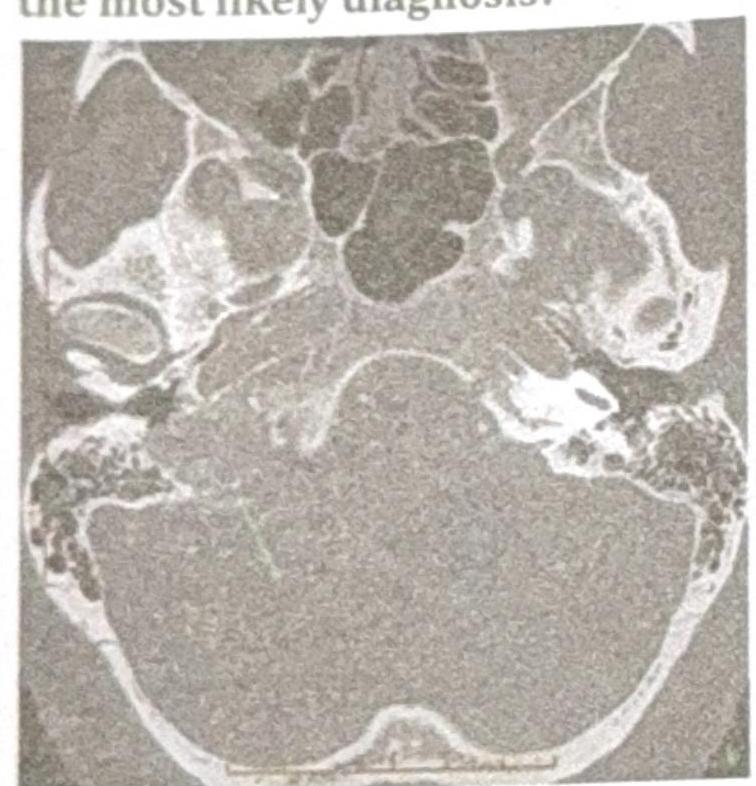
A patient presents with conductive hearing loss, pulsatile tinnitus, and a positive Phelps sign. Based on the CT scan image provided, what is the most likely diagnosis?
Gelle's test is done in?
Positive Rinne test is seen in -
Most difficult site to remove cholesteatoma from the sinus tympani is related to:
Columellar tympanoplasty is -
All of the following techniques are used to control bleeding from bone during mastoid surgery except:
Picket fence fever is a feature of -
Iatrogenic traumatic facial nerve palsy is MOST commonly produced during which of the following surgical procedures?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app