
Otology — MCQs

On this page
What is the most common cause of facial nerve palsy?
65-year-old person with hearing loss with normal speech discrimination is suffering from?
Fenestration operation is which type of tympanoplasty?
What is the surgical procedure for widening of the cartilaginous part of the external auditory canal?
What is the recommended treatment for deafness associated with attic-antral perforation?
Hyperacusis is associated with all of the following conditions except:
Regarding the stapedial reflex, which of the following is true?
Schwartze sign is seen in:
Prussak's space is bounded below by which structure?
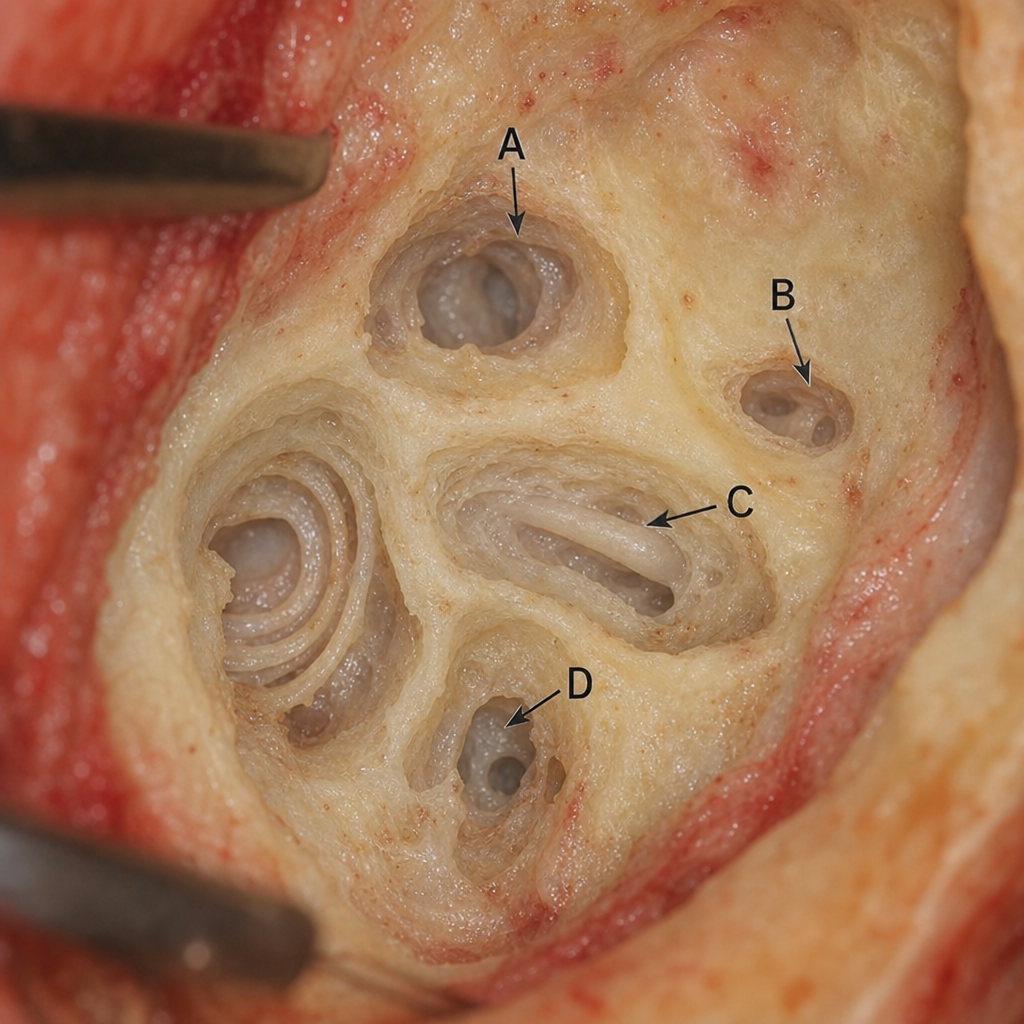
Which of the following marked arrows represents the lateral semicircular canal during a cortical mastoidectomy?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app