
Otology — MCQs

On this page
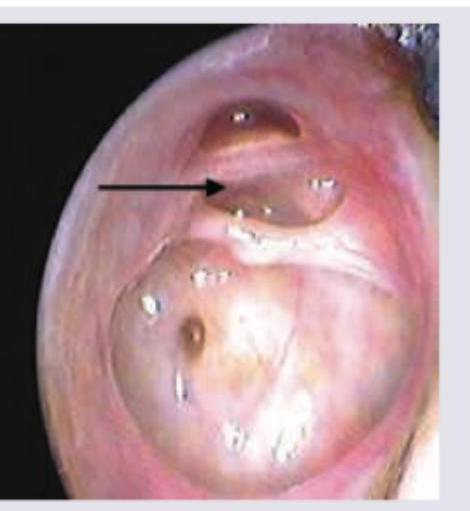
A 20-year-old woman presents with history of scanty ear discharge since childhood. While cleaning the ear today she had bleeding and came to OPD. Otoscopic examination was performed and is shown below. All are true about the condition shown except:
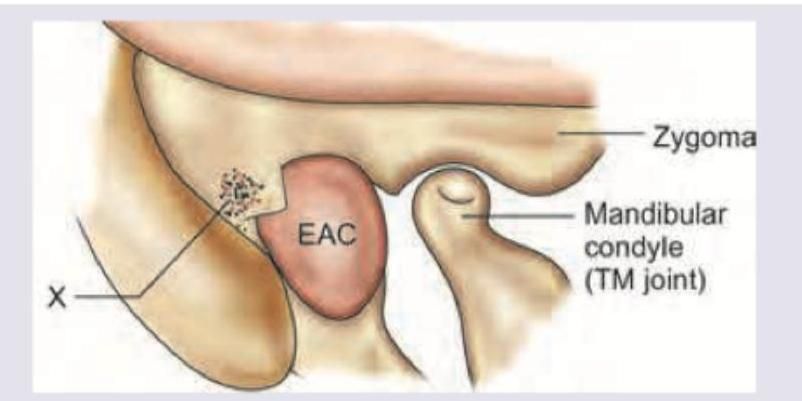
Identify the triangle marked as X in the figure.
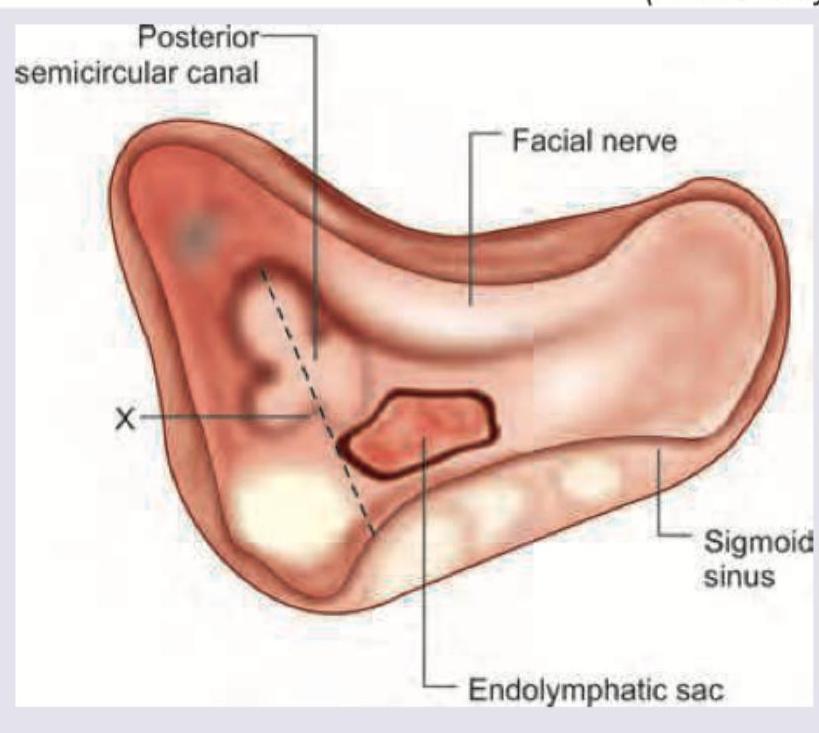
Identify the line shown in the given image:
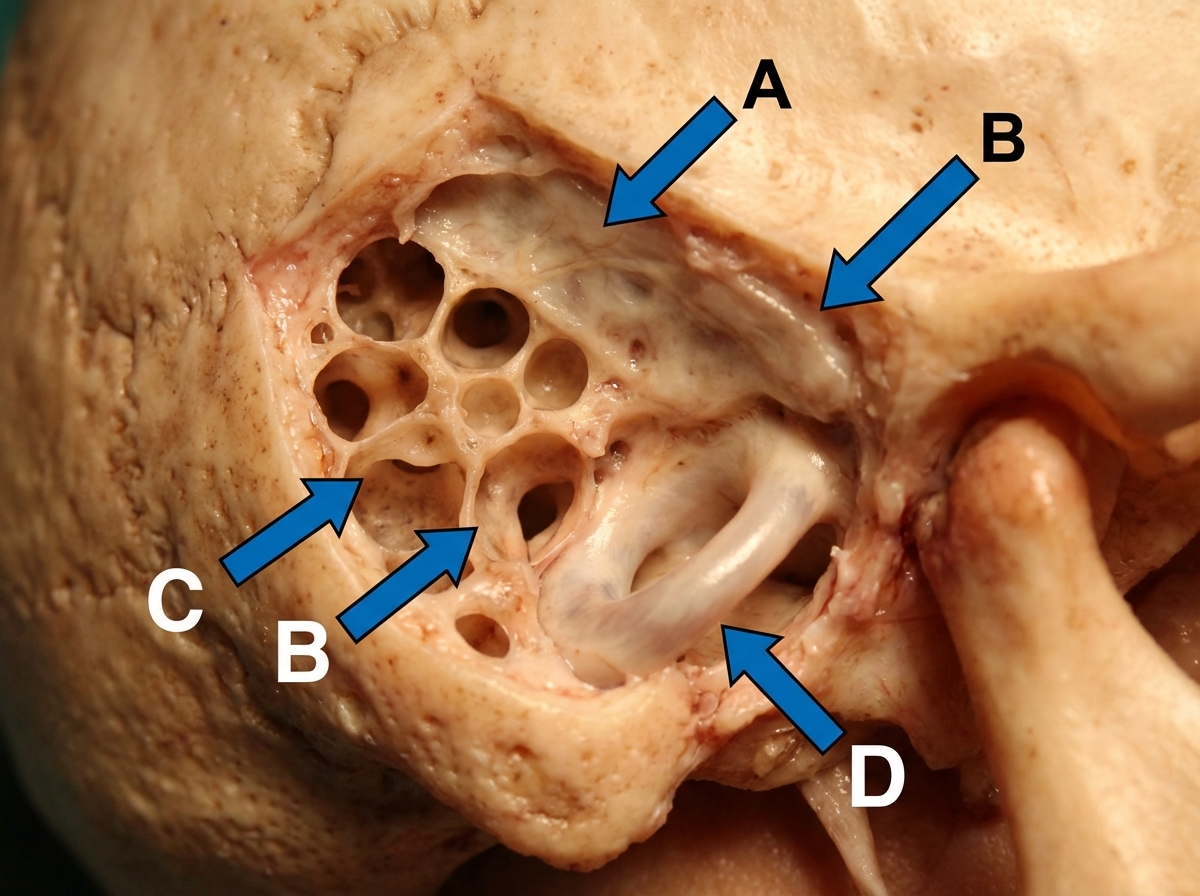
A gross anatomical dissection of the temporal bone is shown. Identify the lateral semi-circular canal. (AIIMS Nov 2017)
A female patient presents with mild conductive hearing loss (CHL) and tinnitus. Based on the pure tone audiometry (PTA) shown in the image, what is the most likely diagnosis?
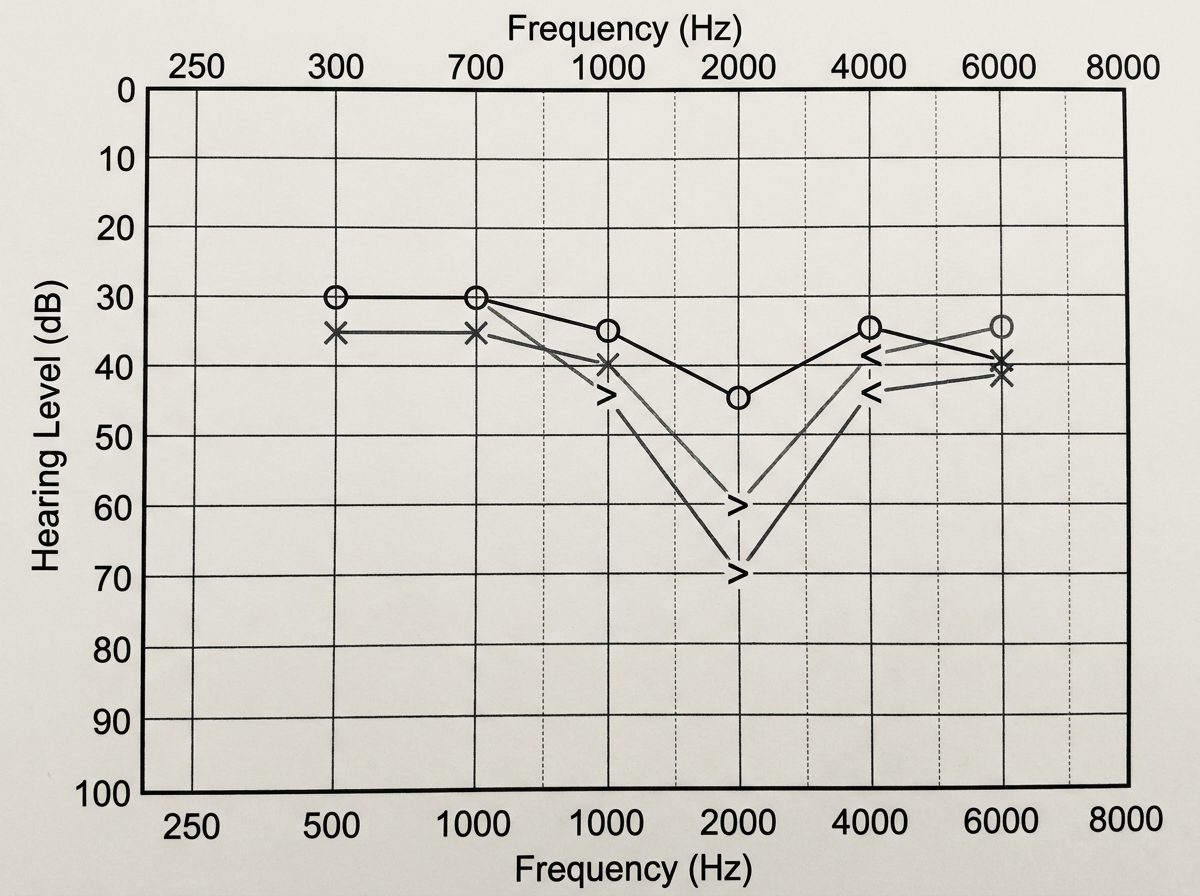
A female patient's pure tone audiometry (PTA) findings show the presence of a Carhart's notch. Which of the following specific clinical signs can be seen in this patient?
Gelle's test is done in?
A pure tone audiogram showing a bone conduction dip (Carhart notch) at 2000 Hz is characteristic of-
All are true about Mastoid antrum except
Nerve most commonly damaged in radical mastoidectomy is -
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app