
Otology — MCQs

On this page
Mastoid reservoir phenomenon is positive in which of the following conditions?
Which of the following is true about Glomus-jugulare tumors?
What is the most common congenital dysplasia of the ear?
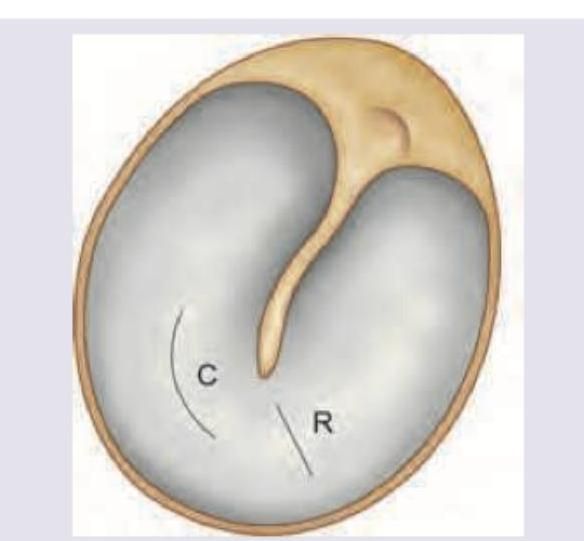
Identify the treatment option with the image given below:
A 35-year-old woman presented to the clinic with the symptoms of hearing loss and pulsatile tinnitus. Further examination reveals conductive hearing loss with the Rinne test negative. A reddish mass is seen behind the tympanic membrane. What is the most likely diagnosis for this patient?
A patient presents to the clinic with a history of chronic ear drainage and hearing loss for several months. Otoscopic examination reveals a central perforation of the tympanic membrane. Pure tone audiometry confirms a conductive hearing loss. Based on these findings, what is the most appropriate next step in the definitive management of this patient's condition?
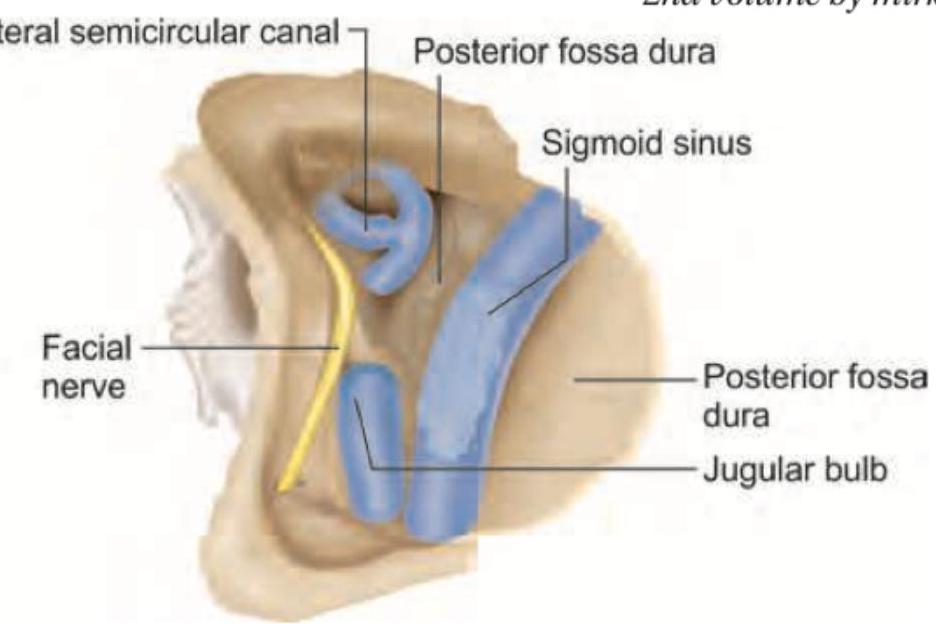
Identify the structure marked in the given image:
All of the following statements regarding this instrument are true except: (Recent NEET Pattern 2016-17)

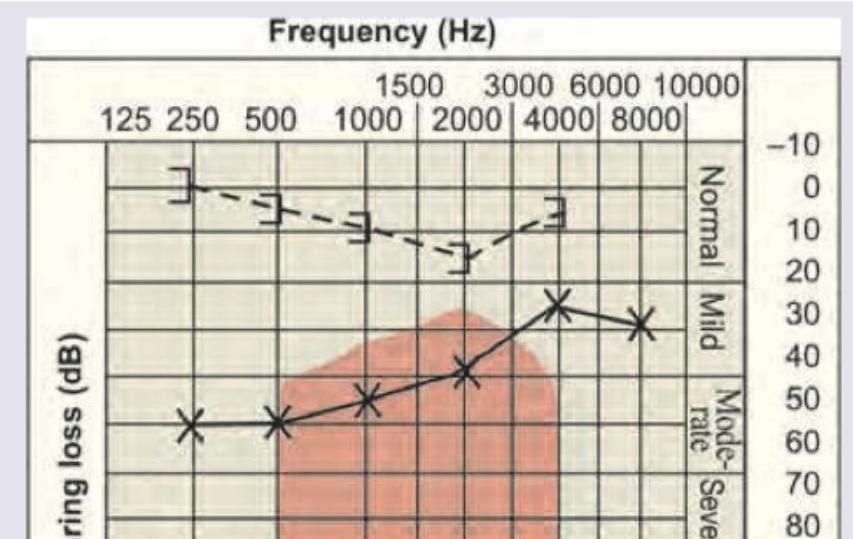
A 25-year-old male complains of difficulty in hearing which has been worsening over last 6 months with occasional tinnitus. Otoscopy shows normal tympanic membrane. Pure tone audiometry shows following recording. What is the diagnosis?
Which of the following is a contraindication to the procedure shown below?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app