
Otology — MCQs

On this page
Tympanoplasty is mainly used for which condition?
In stapedotomy, which of the following is removed?
Which is the narrowest part of the middle ear?
All are features of otosclerosis EXCEPT?
The crus commune is a part of which structure?
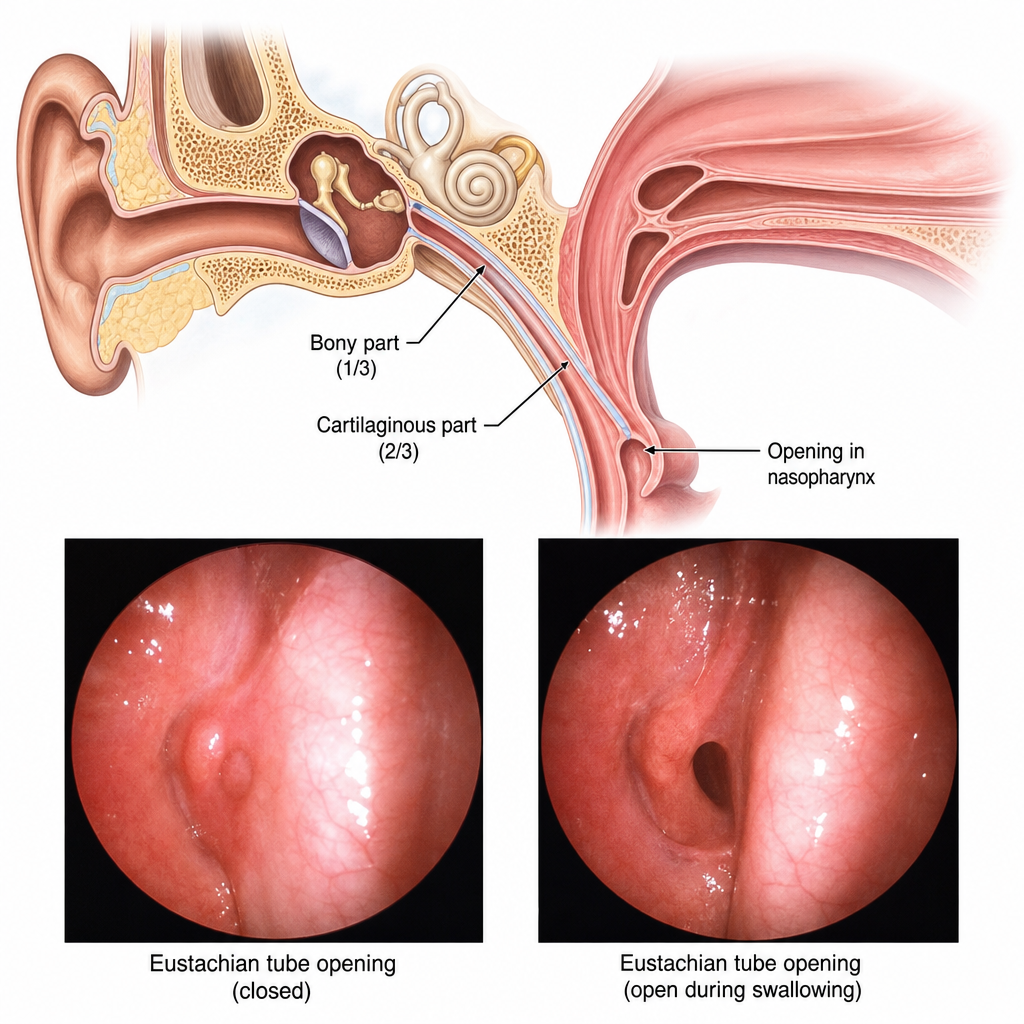
Which of the following statements is true about the Eustachian tube? (a) Length is approximately 36 mm. (b) It is shorter and more vertical in adults. (c) Tensor veli palatini is the main dilator. (d) It opens into the oropharynx. (e) It is lined by ciliated columnar epithelium.
Which anatomical structure appears as a promontory in the middle ear?
The secondary tympanic membrane is present over which anatomical structure?
Which of the following statements are true about otosclerosis?
Which graft is commonly used for tympanoplasty?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app