
Otology — MCQs

On this page
In monaural diplacusis, where is the lesion located?
Which of the following is not resected in stapedotomy?
Glomus jugulare tumors are typically found in relation to which middle ear space?
The most common cause of cerebrospinal otorrhoea is?
Which of the following is NOT true about otosclerosis?
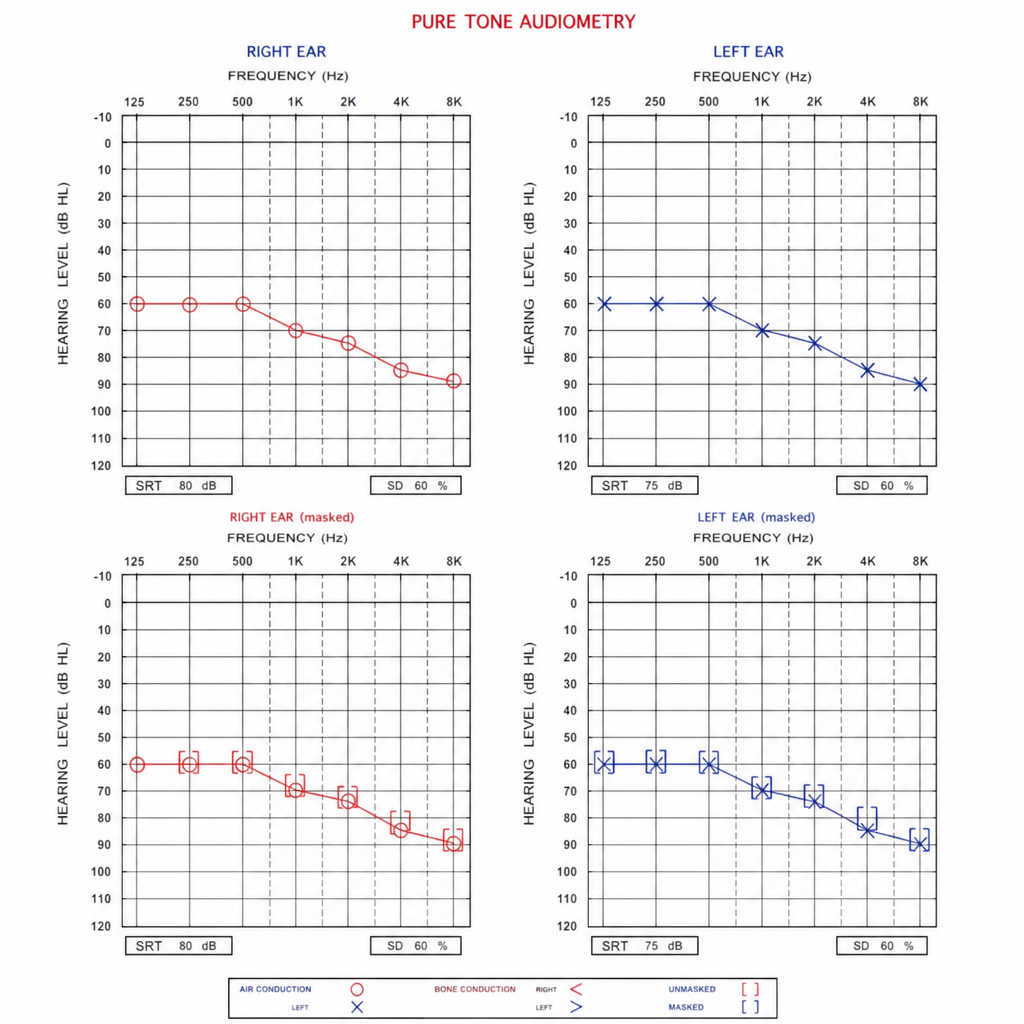
A young adult presents with bilateral severe sensorineural hearing loss. Audiogram shows bilateral pure-tone averages of 90 dB HL with no significant air-bone gap. The patient has trialled bilateral hearing aids for 6 months with poor aided speech recognition scores (<30% on sentence testing in quiet). What management option is most appropriate?
The Tobey-Ayer test is positive in which of the following conditions?
What is the recommended treatment for middle ear papilloma?
Infection of the Central Nervous System spreads to the inner ear through which of the following structures?
Which of the following is a feature of otosclerosis?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app