
Otology — MCQs

On this page
What is the classification system most commonly used for facial nerve injury?
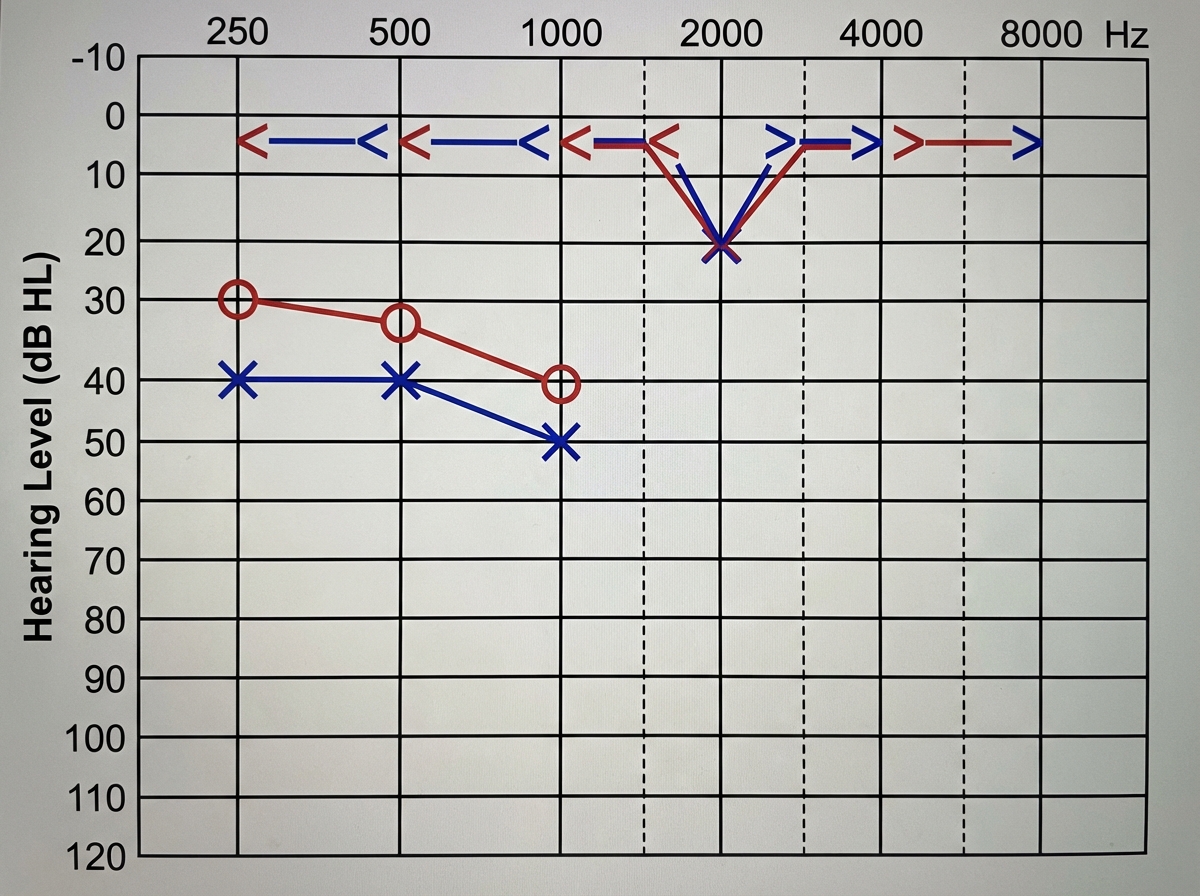
A 28-year-old female presents with a history of bilateral hearing loss and tinnitus. She reports hearing better in noisy environments. Examination reveals intact ear drums bilaterally, and the Rinne test is negative bilaterally. Pure tone audiometry findings are provided below. What is the most probable diagnosis?
The cough response elicited while cleaning the external ear canal is mediated by stimulation of which nerve?
Schwartz sign is seen in which condition?
A child presents to the emergency department with signs of meningeal irritation, following a history of suppurative otitis media in the preceding week. Through which route can infection of the middle ear spread to the central nervous system?
Practice by Chapter
Tympanic Membrane Perforation
Practice Questions
Cholesteatoma
Practice Questions
Tympanoplasty Techniques
Practice Questions
Ossicular Chain Reconstruction
Practice Questions
Mastoidectomy
Practice Questions
Stapedectomy
Practice Questions
Implantable Hearing Devices
Practice Questions
Congenital Aural Atresia
Practice Questions
Otologic Trauma
Practice Questions
Glomus Tumors
Practice Questions
Facial Nerve Decompression
Practice Questions
Rehabilitative Audiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app