
Diseases of the Oral Cavity and Salivary Glands — MCQs

On this page
Acute non-suppurative sialadenitis is most commonly seen in which condition?
What is Epulis?
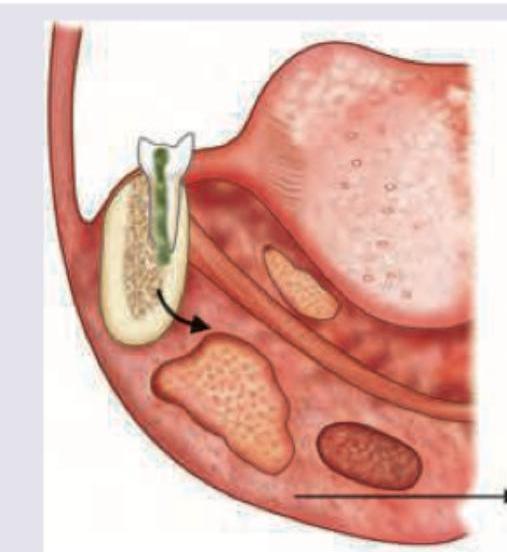
During the extraction of an upper first molar, the mesiobuccal root is missing and suspected to have been pushed into the maxillary sinus. What is the recommended method to determine antral perforation?
Which is incorrect about the instrument shown?

A patient with dental caries has developed a swelling in the area shown in the image. Diagnosis is:
A 16-year-old patient complains of difficulty in swallowing, difficulty in talking and sometimes difficulty in breathing. On physical examination the presentation is similar to that shown in the picture. What would be the probable diagnosis?

A 6-year-old boy has recurrent history of pain and swelling below his left ear, which generally lasts for 3–7 days and improves mildly after a course of antibiotics. Sialography shows punctate sialectasis. He should be treated by
What is a clinical feature of mouth breathing?
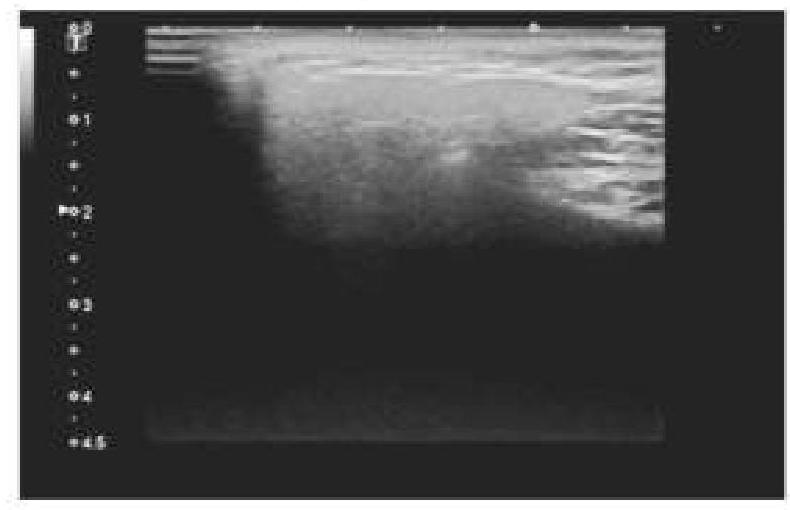
A 45-year-old patient complained of pain on one side of the neck. She is afraid of eating food as it worsens the pain. An ultrasound of the salivary glands is shown below. What is the most likely diagnosis?
Which anatomical location is often referred to as the 'graveyard of the ENT surgeon' due to its association with undetected malignancies?
Practice by Chapter
Stomatitis
Practice Questions
Oral Ulcers
Practice Questions
Oral Leukoplakia
Practice Questions
Oral Cancers
Practice Questions
Sialadenitis
Practice Questions
Sialolithiasis
Practice Questions
Salivary Gland Tumors
Practice Questions
Ranula
Practice Questions
Xerostomia
Practice Questions
Sjögren's Syndrome
Practice Questions
Oral Manifestations of Systemic Diseases
Practice Questions
Temporomandibular Joint Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app