
Diseases of the Oral Cavity and Salivary Glands — MCQs

On this page
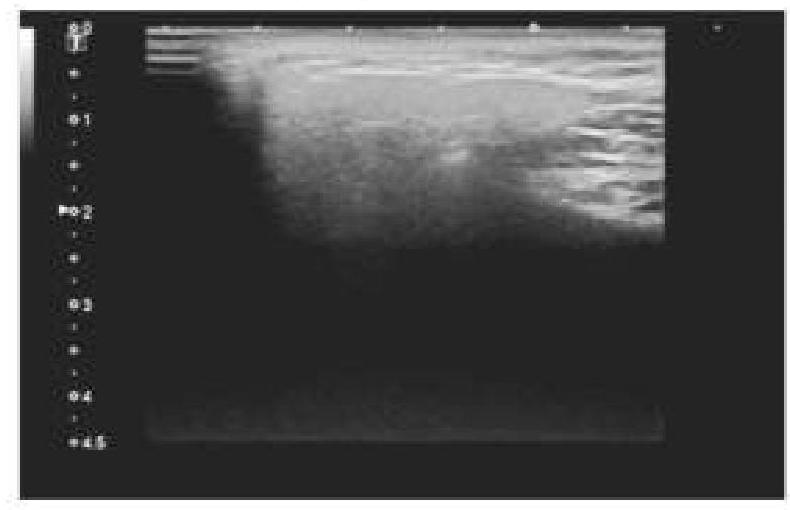
A 45-year-old patient complained of pain on one side of the neck. She is afraid of eating food as it worsens the pain. An ultrasound of the salivary glands is shown below. What is the most likely diagnosis?
Not typically associated with Ludwig's angina is
What does sialosis refer to?
Practice by Chapter
Stomatitis
Practice Questions
Oral Ulcers
Practice Questions
Oral Leukoplakia
Practice Questions
Oral Cancers
Practice Questions
Sialadenitis
Practice Questions
Sialolithiasis
Practice Questions
Salivary Gland Tumors
Practice Questions
Ranula
Practice Questions
Xerostomia
Practice Questions
Sjögren's Syndrome
Practice Questions
Oral Manifestations of Systemic Diseases
Practice Questions
Temporomandibular Joint Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app