
Diseases of the Oral Cavity and Salivary Glands — MCQs

On this page
A 50-year-old smoker presents to the hospital with a painless oral lesion and white patch that develops in the oral cavity, as shown in the image. The white plaque cannot be scraped off. What is the diagnosis?
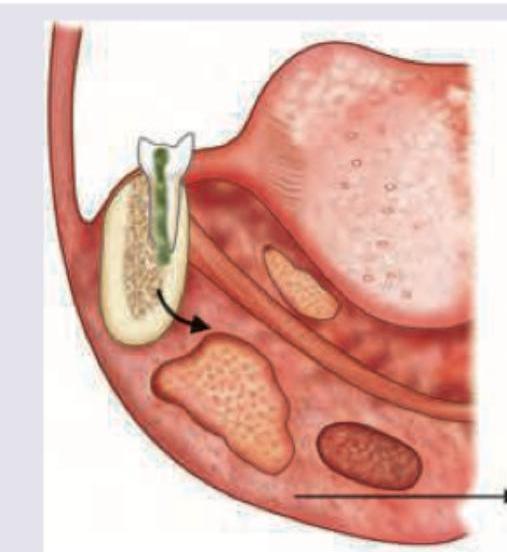
A patient with dental caries has developed a swelling in the area shown in the image. Diagnosis is:
A 16-year-old patient complains of difficulty in swallowing, difficulty in talking and sometimes difficulty in breathing. On physical examination the presentation is similar to that shown in the picture. What would be the probable diagnosis?

A male patient complains of trismus, dysphagia and respiratory distress. On examination, he has a submental swelling with fever, tachycardia and tachypnea. What is the most likely diagnosis?

A 6-year-old boy has recurrent history of pain and swelling below his left ear, which generally lasts for 3–7 days and improves mildly after a course of antibiotics. Sialography shows punctate sialectasis. He should be treated by
A 22 year old male addicted to alcohol and abused with pan-masala-arecanut comes to the clinic with limited mouth opening and restricted tongue movement. The clinical suspicion will be of:
Cause of Ludwig angina is:
Commonest cause of Ludwig's Angina is
Symmetrical persistent enlargement of the parotid gland is seen in:
Sialolithiasis is most commonly seen in which gland?
Practice by Chapter
Stomatitis
Practice Questions
Oral Ulcers
Practice Questions
Oral Leukoplakia
Practice Questions
Oral Cancers
Practice Questions
Sialadenitis
Practice Questions
Sialolithiasis
Practice Questions
Salivary Gland Tumors
Practice Questions
Ranula
Practice Questions
Xerostomia
Practice Questions
Sjögren's Syndrome
Practice Questions
Oral Manifestations of Systemic Diseases
Practice Questions
Temporomandibular Joint Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app