
Diseases of the Oral Cavity and Salivary Glands — MCQs

On this page
Mucous retention cysts are most commonly found on which anatomical location?
What is the most common cause of trismus due to infection in a muscle?
What is the treatment for a child with cherubism?
A businessman notices a lump in front of his ear while shaving. His wife thinks it has been present for several months. What is the most likely cause of a mass in the parotid gland in this patient?
A painless, fluid-filled retention cyst appearing in an area of recent dental treatment may be the result of which of the following?
Which of the following statements is false regarding plunging ranula?
A palatal abscess most commonly results from an infection of which of the following teeth?
Leukoplakia with the worst prognosis is typically found on which of the following locations?
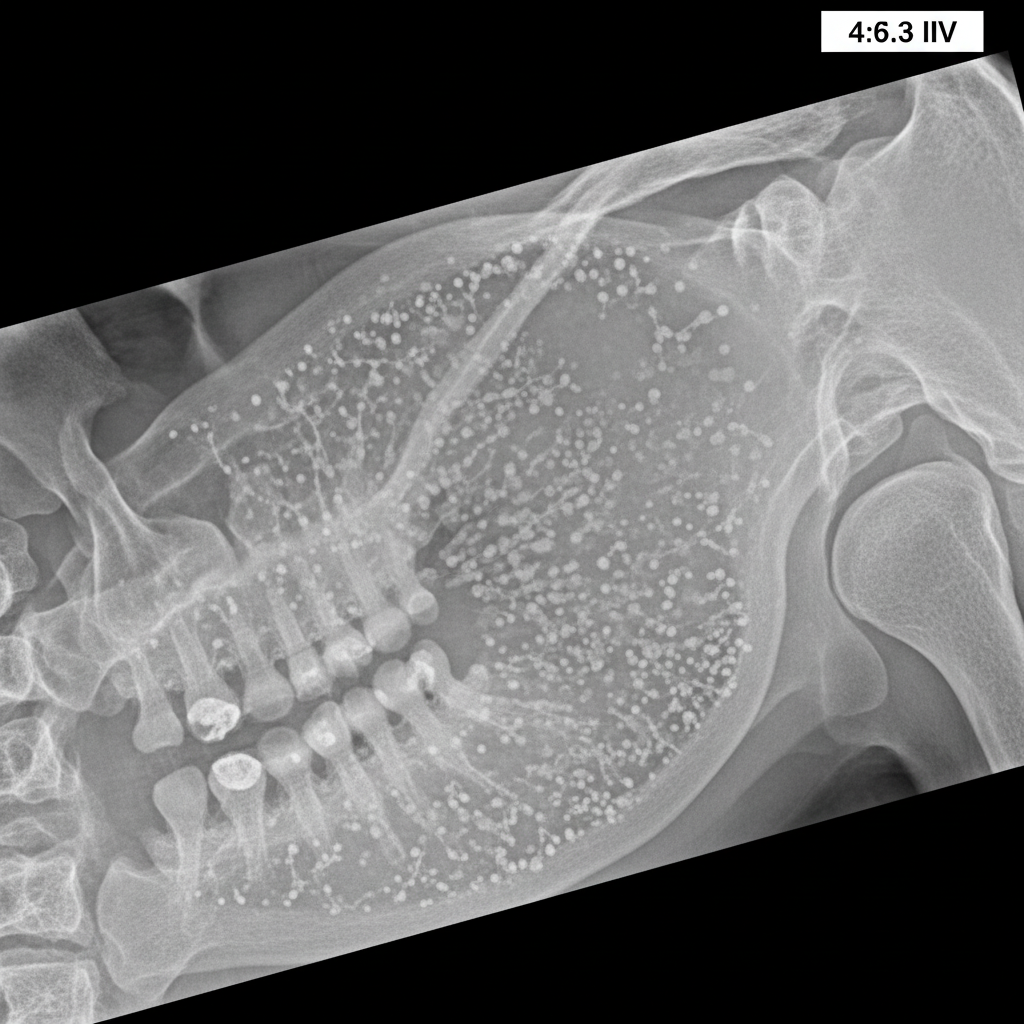
A sialography report of a 46-year-old female is provided. Based on the findings, what is the most likely diagnosis?
What is the characteristic ENT manifestation of Peutz-Jeghers syndrome with benign intestinal polyps?
Practice by Chapter
Stomatitis
Practice Questions
Oral Ulcers
Practice Questions
Oral Leukoplakia
Practice Questions
Oral Cancers
Practice Questions
Sialadenitis
Practice Questions
Sialolithiasis
Practice Questions
Salivary Gland Tumors
Practice Questions
Ranula
Practice Questions
Xerostomia
Practice Questions
Sjögren's Syndrome
Practice Questions
Oral Manifestations of Systemic Diseases
Practice Questions
Temporomandibular Joint Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app