
Diseases of the Oral Cavity and Salivary Glands — MCQs

On this page
Which of the following is NOT a premalignant lesion of the oral cavity?
Which tumor does not occur in minor salivary glands?
Which of the following is false regarding pleomorphic adenoma?
Which of the following is NOT a treatment option for chronic submucosal fibrosis?
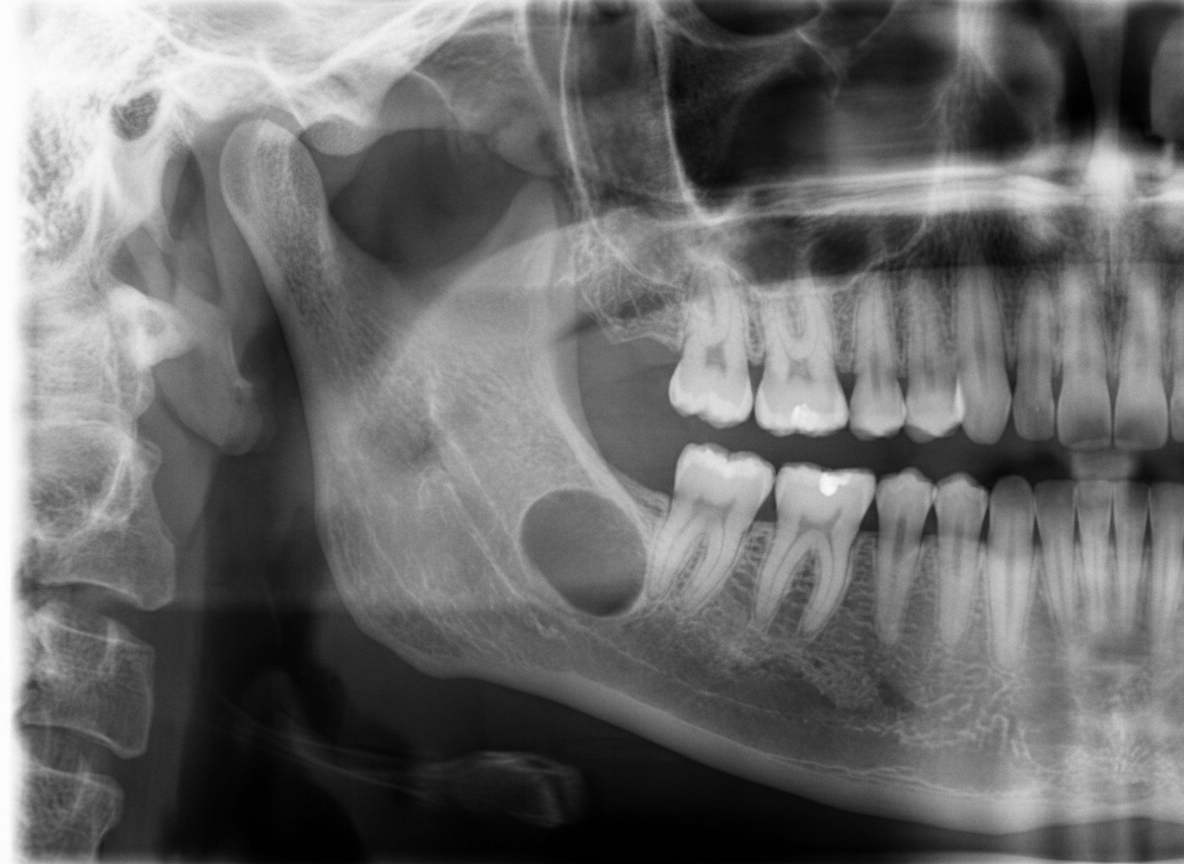
A 45-year-old male presented for a routine dental checkup. All teeth in the lower right quadrant were vital. A panoramic radiograph was taken. Which of the following can be the most probable diagnosis?
Stones in the distal portion of Wharton's duct are best visualized by which radiographic view?
What is the condition involved with an unerupted or impacted tooth?
What is the investigation of choice for parotid gland calculi?
Which of the following is NOT typically a white lesion found in the oral cavity?
Which of the following is NOT a precancerous lesion of the oral cavity?
Practice by Chapter
Stomatitis
Practice Questions
Oral Ulcers
Practice Questions
Oral Leukoplakia
Practice Questions
Oral Cancers
Practice Questions
Sialadenitis
Practice Questions
Sialolithiasis
Practice Questions
Salivary Gland Tumors
Practice Questions
Ranula
Practice Questions
Xerostomia
Practice Questions
Sjögren's Syndrome
Practice Questions
Oral Manifestations of Systemic Diseases
Practice Questions
Temporomandibular Joint Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app