
Psoriasis — MCQs

On this page
Auspitz sign is seen in which of the following conditions?
A 50-year-old patient presents with erythematous scaly plaques over the trunk and extremities for the last 10 years. The lesions are occasionally itchy, with a history of remission and relapse, and exacerbation during winters. What is the most likely diagnosis?
Which of the following is NOT a treatment option for psoriasis?
Which of the following conditions is associated with Psoriasis?
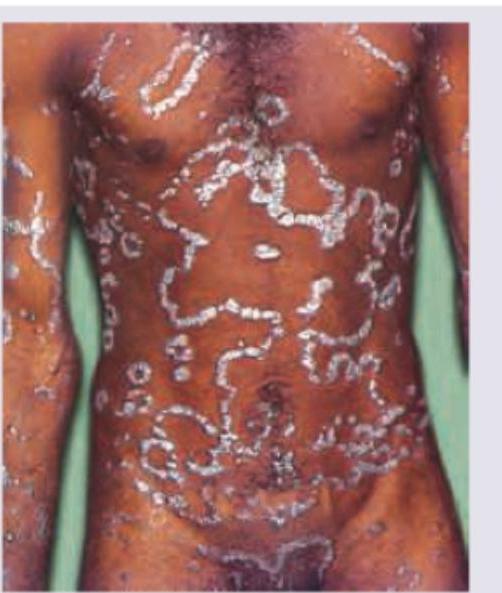
A child with a sore throat starts developing skin lesions as in the image below. Which of the following is the diagnosis?

A 26-year-old male presented with erythematous plaques covered with silvery scales over the extensor surfaces of both arms. Punctate pitting was noted on examining the nails. What is the most likely diagnosis?
All are correct about the condition shown except:
Choose the correct statement for the clinical sign shown in psoriasis: (Recent NEET Pattern 2016-17)

A patient presents with the skin lesions shown in the image. All of the following are routinely indicated for the treatment of this condition EXCEPT:

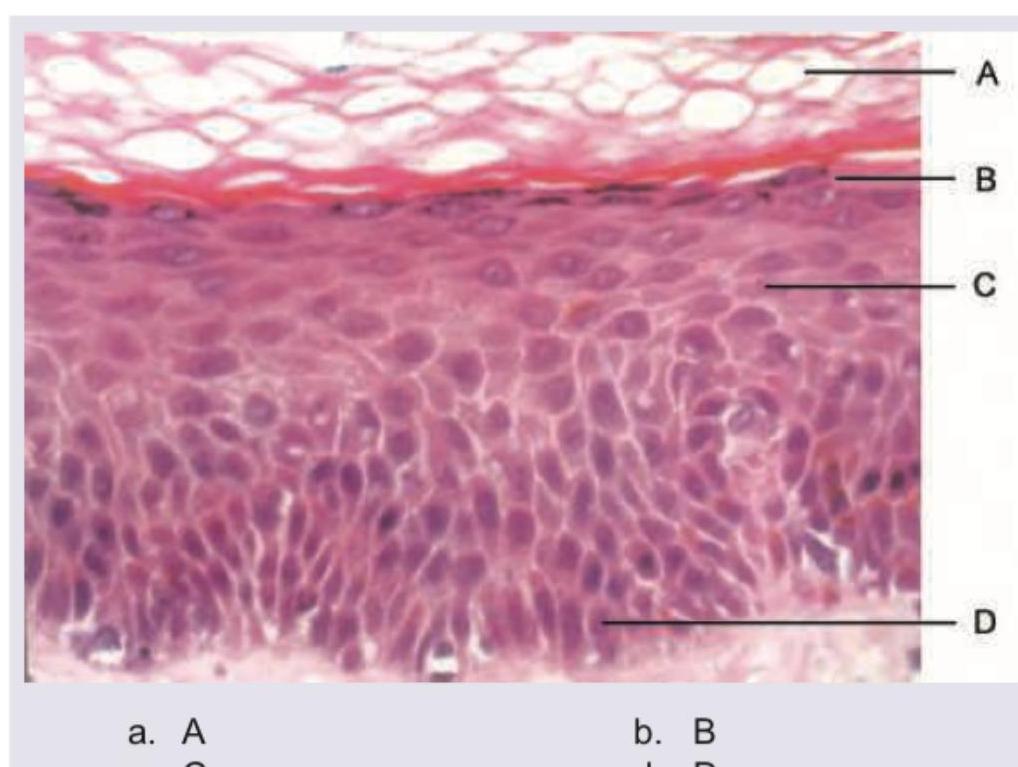
Which of the following layers is typically diminished or absent beneath areas of parakeratosis in psoriasis?
Practice by Chapter
Pathophysiology of Psoriasis
Practice Questions
Psoriasis Vulgaris
Practice Questions
Guttate Psoriasis
Practice Questions
Erythrodermic Psoriasis
Practice Questions
Pustular Psoriasis
Practice Questions
Palmoplantar Psoriasis
Practice Questions
Nail Psoriasis
Practice Questions
Scalp Psoriasis
Practice Questions
Psoriatic Arthritis
Practice Questions
Topical Therapy for Psoriasis
Practice Questions
Systemic Therapy for Psoriasis
Practice Questions
Phototherapy and Biologics for Psoriasis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app