
Pediatric Dermatology — MCQs

On this page
The diagnosis of the child shown in the image is:
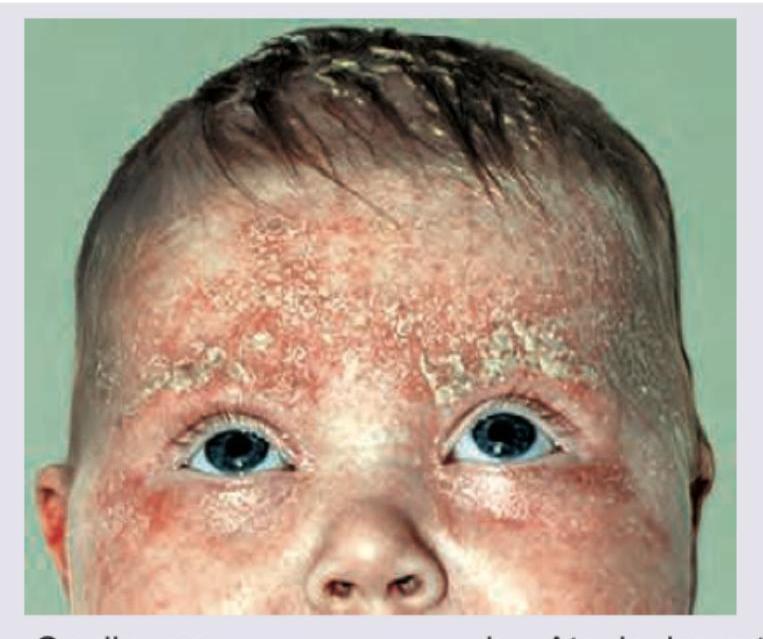
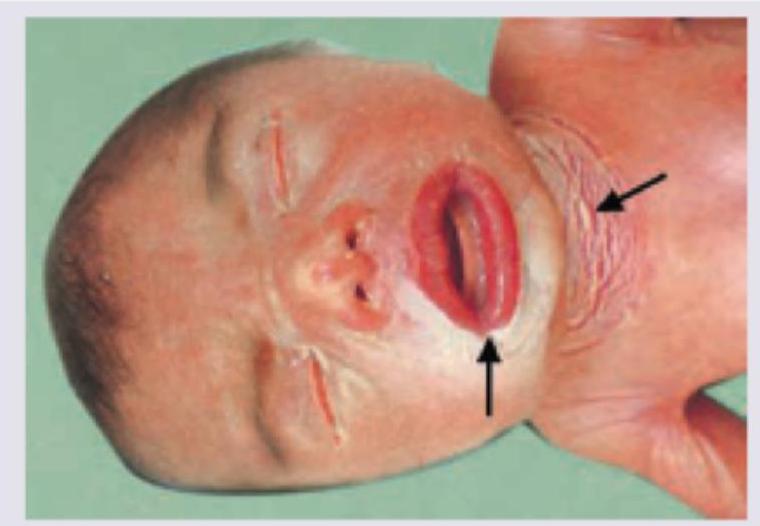
The image shows a newborn with characteristic skin findings. What is the most likely diagnosis?
Identify the neurocutaneous disorder.

Consider the following in respect of Salmon patch : 1. It is a hemangioma. 2. Its usual site is nape of neck. 3. It is common in children. 4. It needs surgical excision. Which of the statements given above are correct ?
A child presented with asymptomatic lesions on the forearm and on the shaft of the penis. The lesions on the forearm are shown below. What is the most likely diagnosis?

A 5-month-old child presented to the dermatology OPD with dryness along with white, fine scales on most parts of the body with sparing of face. The child was born at 39 weeks gestation by spontaneous vaginal delivery outside the hospital. On examination, fine, white scales were observed predominantly on the extensor surfaces of the limbs along with characteristic hyperlinearity of palms and accentuation of skin markings. Which of the following genes is most likely defective in the above condition:
Earliest feature of Tuberous sclerosis is:
Acrodermatitis enteropathica is associated with deficiency of?
Which of the following diseases of the skin is the most likely to be associated with partial anodontia?
Baby born with membrane around him at the time of birth. Which of the following conditions is depicted?
Practice by Chapter
Neonatal Dermatology
Practice Questions
Infantile Hemangiomas and Vascular Malformations
Practice Questions
Atopic Dermatitis in Children
Practice Questions
Acne in Childhood and Adolescence
Practice Questions
Childhood Exanthems
Practice Questions
Genetic Skin Disorders in Children
Practice Questions
Genodermatoses
Practice Questions
Nutritional Dermatoses in Children
Practice Questions
Pigmentary Disorders in Children
Practice Questions
Hair Disorders in Children
Practice Questions
Child Abuse: Cutaneous Manifestations
Practice Questions
Therapeutic Considerations in Pediatric Dermatology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app