
Pediatric Dermatology — MCQs

On this page
A neonate presents with a growing skin lesion, as shown in the image provided. The mother reports that the lesion has been increasing in size daily. What is the appropriate management?
A 6-month-old baby presents with a bright red, raised, soft nodule measuring 2 cm in diameter on the forehead. The lesion has well-defined borders, appeared 2 weeks after birth as a small red spot, and has been growing rapidly over the past few months. The surface has a characteristic strawberry-like appearance with a lobulated texture. What is the most likely diagnosis?
A neonate presents with blotchy rash on the abdomen as shown in the image. What is the diagnosis?

A 1-year-old unimmunised child with HbsAg positivity is having following skin lesions. What is the diagnosis?

An 8-year-old boy who was diagnosed with hypertrophic cardiomyopathy has reddish papules all over the body developing after birth. He also complains of severe pain in hands and feet. Which of the following is correct?
An 8-year-old girl has extreme photosensitivity since birth. She has recently been diagnosed with skin cancer. What is the diagnosis?
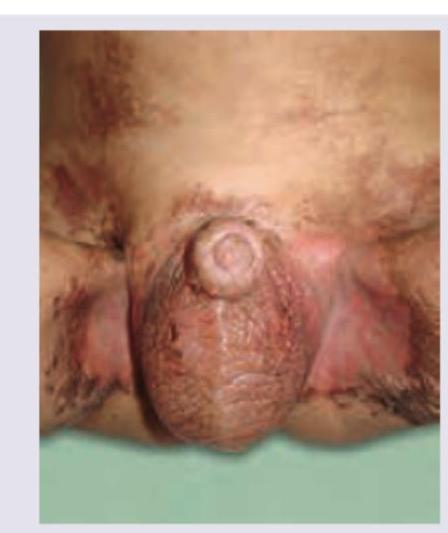
A 7-month-old child after weaning develops diarrhea and following skin lesions. The lesions did not respond to topical clotrimazole. All are true about the condition except:
All are true about this lesion seen in a child with epilepsy except:

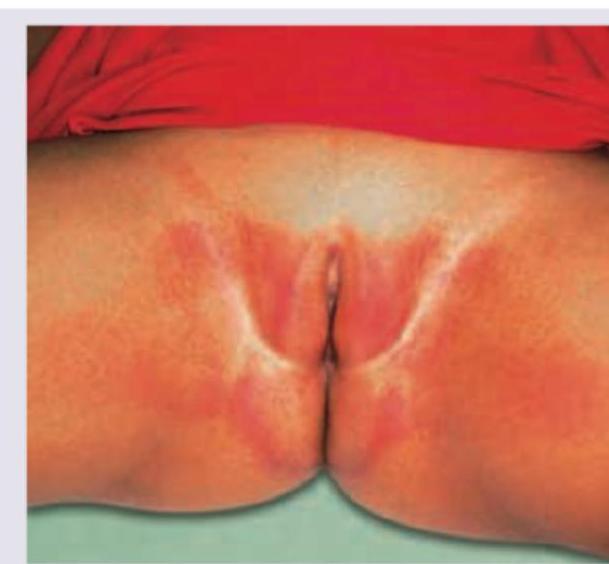
A 6-month-old infant presents with a rash in the diaper area. On examination, erythema and erosions are noted on the convex surfaces (labia and buttocks), while the skin folds are relatively spared. The infant has not grown out of diapers yet. Based on the clinical image, what is the most likely diagnosis?
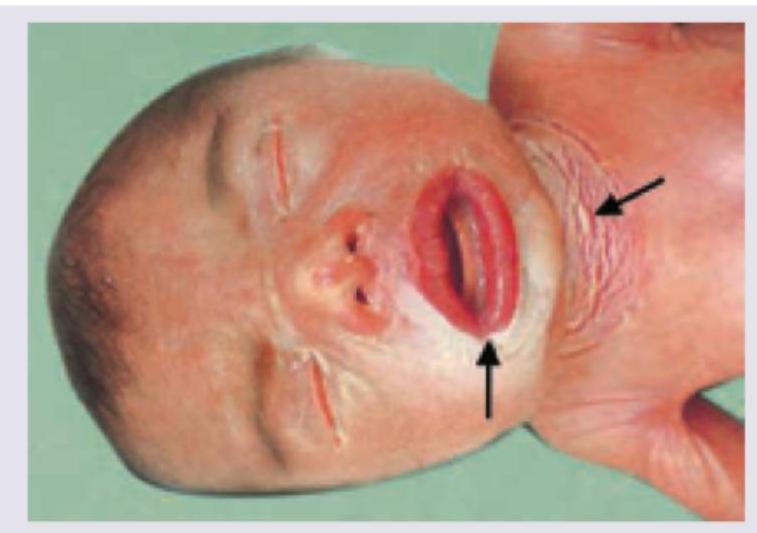
A neonate presents with the condition shown in the image below. This condition has all of the following features EXCEPT:
Practice by Chapter
Neonatal Dermatology
Practice Questions
Infantile Hemangiomas and Vascular Malformations
Practice Questions
Atopic Dermatitis in Children
Practice Questions
Acne in Childhood and Adolescence
Practice Questions
Childhood Exanthems
Practice Questions
Genetic Skin Disorders in Children
Practice Questions
Genodermatoses
Practice Questions
Nutritional Dermatoses in Children
Practice Questions
Pigmentary Disorders in Children
Practice Questions
Hair Disorders in Children
Practice Questions
Child Abuse: Cutaneous Manifestations
Practice Questions
Therapeutic Considerations in Pediatric Dermatology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app