
Blistering Diseases — MCQs

On this page
A patient presents with intensely pruritic vesicular lesions on extensor surfaces. What is the most likely diagnosis based on the clinical image?

All are true about the lesion shown in a patient with stunting, osmotic diarrhea and anemia except:

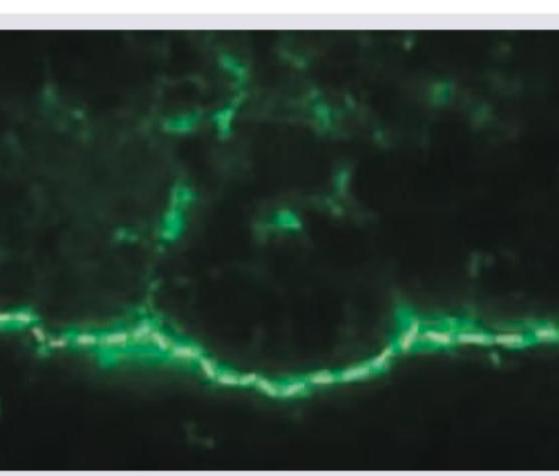
Which of the following vesico-bullous disorders will exhibit the direct immunofluorescence shown below?
Identify the lesion shown below.

A 60-year-old female presents with eczematous itching lesions. Biopsy revealed a subepidermal cleft with Direct Immunofluorescence showing Linear C3 & IgG deposition along the basement membrane zone. What is the likely diagnosis?
A 4-year-old boy presents with multiple vesicles and bullae on an erythematous base. The lesions primarily affect his elbows, knees, and buttocks, with some oral involvement. His mother reports that he gets similar lesions with minor trauma. Skin biopsy shows subepidermal separation with neutrophilic infiltrate. Direct immunofluorescence shows linear IgA deposits at the basement membrane. Which of the following is the most appropriate treatment?
In congenital dystrophic variety of epidermolysis bullosa, mutation is seen in the gene coding for:
All of the following statements about Stevens-Johnson Syndrome are true EXCEPT:
A patient with acute history of blistering and denudation involving >30% BSA along with erosions of the lips with hemorrhagic crusting and other mucosa for few days. What is the most common triggering factor?
A diabetic patient presents with painful hemorrhagic bullae on legs. Investigations show raised creatinine. Most likely diagnosis:
Practice by Chapter
Pemphigus Vulgaris
Practice Questions
Pemphigus Foliaceus
Practice Questions
Bullous Pemphigoid
Practice Questions
Cicatricial Pemphigoid
Practice Questions
Dermatitis Herpetiformis
Practice Questions
Epidermolysis Bullosa
Practice Questions
Linear IgA Bullous Dermatosis
Practice Questions
Pemphigoid Gestationis
Practice Questions
Drug-Induced Bullous Disorders
Practice Questions
Immunofluorescence in Bullous Diseases
Practice Questions
Management of Autoimmune Bullous Diseases
Practice Questions
Genetic Counseling in Inherited Blistering Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app