
Blistering Diseases — MCQs

On this page
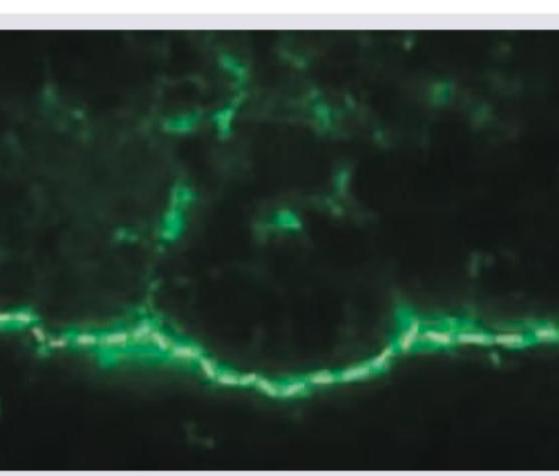
Which of the following vesico-bullous disorders will exhibit the direct immunofluorescence shown below?
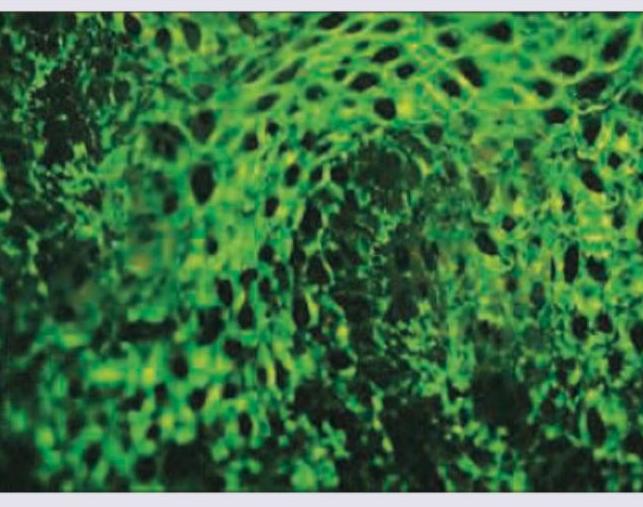
Which of the following vesico-bullous disorders will exhibit the direct immunofluorescence shown below? (Recent NEET Pattern 2016-17)

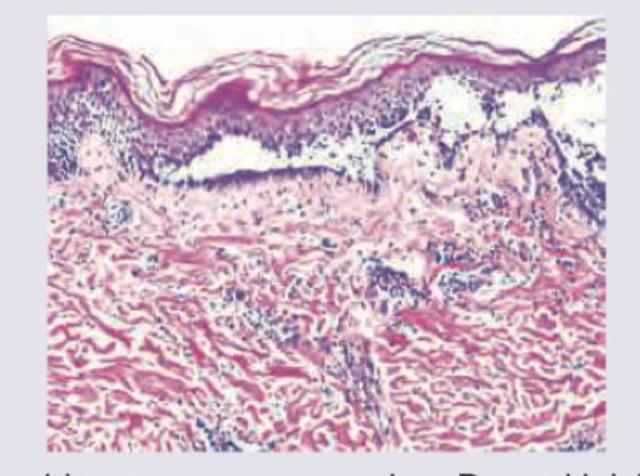
What is the diagnosis based on the image shown below?
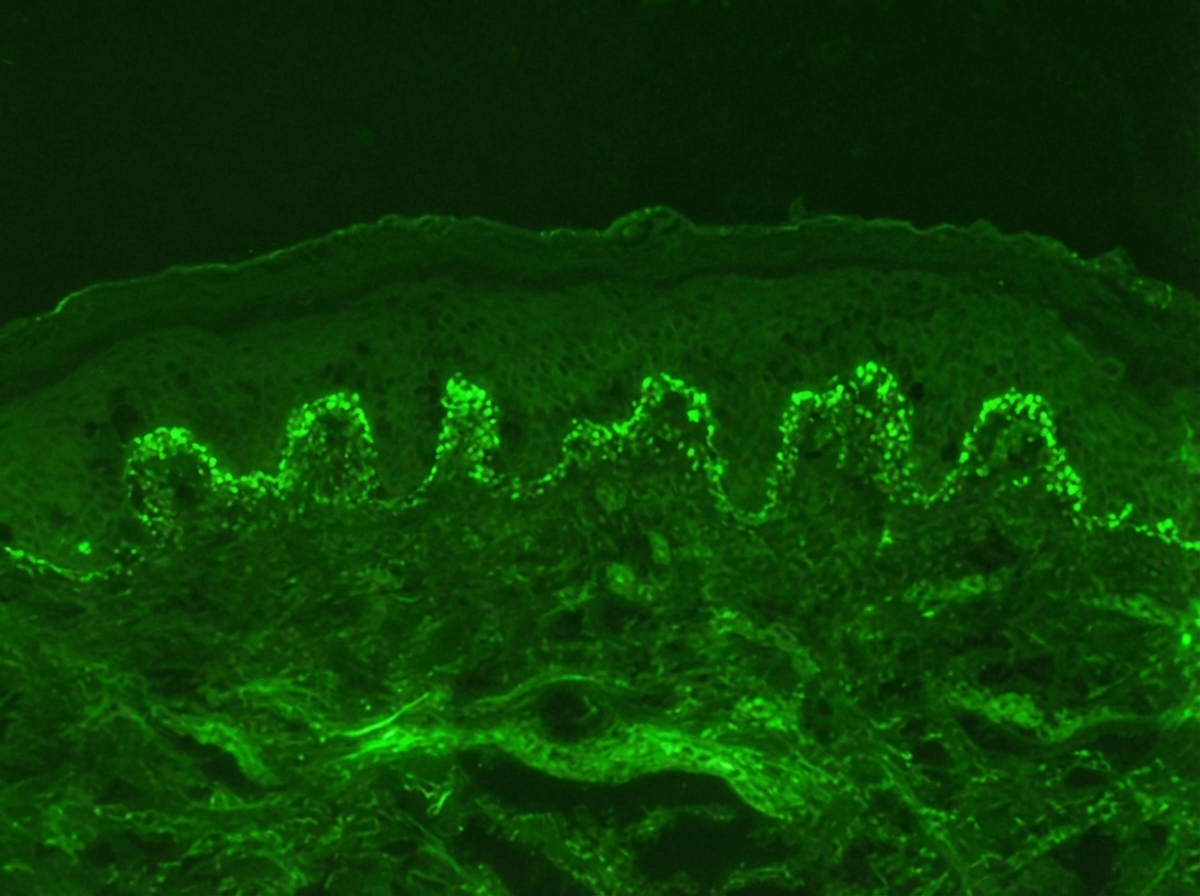
A 25-year-old lady presents with painful blisters in oral mucosa and skin. Direct immune-fluorescence picture is given below. Which of the following is incorrect about the condition shown?
A patient presents with skin lesions and erosions on the buccal mucosa. The immunofluorescence image is shown. What is the most likely diagnosis?
Identify the diagnosis based on the dermatology immunofluorescence (IF) image provided.
A 30-year-old woman presents with flaccid bullae on her skin that are easy to rupture. A biopsy of the lesion reveals a suprabasal split. What is the most likely diagnosis?
A 60-year-old female presents with eczematous itching lesions. Biopsy revealed a subepidermal cleft with Direct Immunofluorescence showing Linear C3 & IgG deposition along the basement membrane zone. What is the likely diagnosis?
Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
A 25-year-old woman presents with multiple tense bullae on her arms and legs that developed over the past week. She reports taking amoxicillin for a sore throat 2 weeks ago. Skin biopsy shows subepidermal bulla formation with linear IgA deposits along the basement membrane. Which of the following is the most appropriate treatment?
Practice by Chapter
Pemphigus Vulgaris
Practice Questions
Pemphigus Foliaceus
Practice Questions
Bullous Pemphigoid
Practice Questions
Cicatricial Pemphigoid
Practice Questions
Dermatitis Herpetiformis
Practice Questions
Epidermolysis Bullosa
Practice Questions
Linear IgA Bullous Dermatosis
Practice Questions
Pemphigoid Gestationis
Practice Questions
Drug-Induced Bullous Disorders
Practice Questions
Immunofluorescence in Bullous Diseases
Practice Questions
Management of Autoimmune Bullous Diseases
Practice Questions
Genetic Counseling in Inherited Blistering Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app