
Blistering Diseases — MCQs

On this page
A patient presents with painful blisters along the chest wall. All of the following tests are useful for diagnosis except:
An elderly patient presents with itchy tense blisters on normal looking skin as well as on urticarial plaques as shown below. The most probable diagnosis is: (AIIMS Nov 2015)

The given picture depicts:

The image shows presence of:
All are true about the lesions shown except:

A patient presents with the skin lesions shown in the image. While evaluating for possible blistering disorders, all of the following conditions could present with similar morphology EXCEPT:

All are true about the lesion shown in the image except:

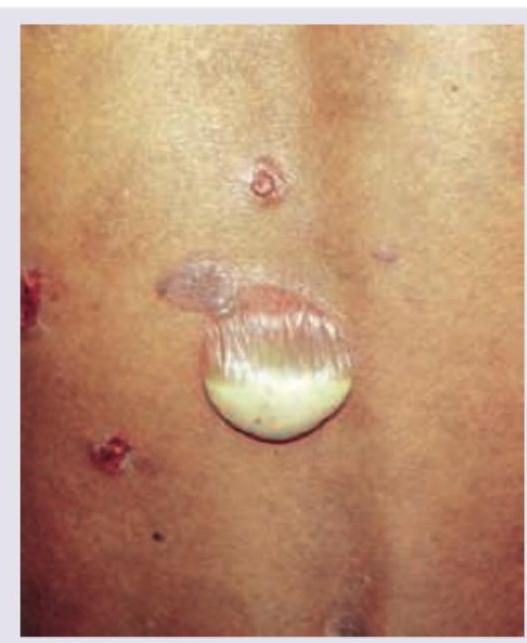
The following image shows a flaccid bulla. This finding is characteristically seen in:
Pseudo Nikolsky sign is seen in all except:
All are true about the lesion shown in a patient with stunting, osmotic diarrhea and anemia except:

Practice by Chapter
Pemphigus Vulgaris
Practice Questions
Pemphigus Foliaceus
Practice Questions
Bullous Pemphigoid
Practice Questions
Cicatricial Pemphigoid
Practice Questions
Dermatitis Herpetiformis
Practice Questions
Epidermolysis Bullosa
Practice Questions
Linear IgA Bullous Dermatosis
Practice Questions
Pemphigoid Gestationis
Practice Questions
Drug-Induced Bullous Disorders
Practice Questions
Immunofluorescence in Bullous Diseases
Practice Questions
Management of Autoimmune Bullous Diseases
Practice Questions
Genetic Counseling in Inherited Blistering Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app