
Prophylaxis and Management — MCQs

Which of the following are treatment options for acne vulgaris?
What is the best way to control the MRSA infection in the ward?
A patient with a non-obstructing carcinoma of the sigmoid colon is being prepared for elective resection. To minimize the risk of postoperative infectious complications, what should be included in your planning?
A boil is due to staphylococcal infection of:
Which of the following disorders would be more likely associated with Staphylococcus saprophyticus rather than Staphylococcus aureus?
A diabetic patient developed cellulitis due to S. aureus, which was found to be methicillin resistant on the antibiotic sensitivity testing. All of the following antibiotics will be appropriate except ?
Hyperkalemia management includes all except:
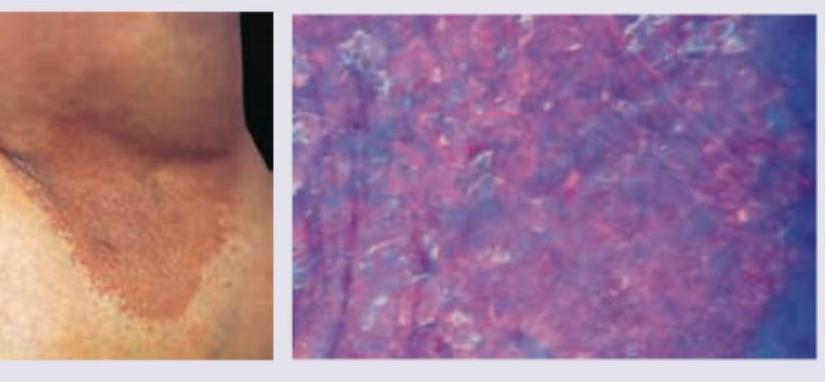
A 35-year-old obese woman presents with recurrent lesions in both axilla in summer season. Wood lamp examination is shown. The diagnosis is:
What is the treatment for granuloma inguinale?
A child presents with grouped vesicles on an erythematous base on the buttocks. What is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app