
Ecthyma — MCQs

What is the diagnosis of an umbilicated, pearly white, asymptomatic skin lesion?
An 18-year-old man has facial and upper back lesions that have waxed and waned for the past 6 years. On physical examination, there are 0.3- to 0.9-cm comedones, erythematous papules, nodules, and pustules most numerous on the lower face and posterior upper trunk. Other family members have been affected by this condition at a similar age. The lesions worsen during a 5-day cruise to the Adriatic. Which of the following organisms is most likely to play a key role in the pathogenesis of these lesions?
A patient, a resident of Himachal Pradesh, presented with a series of ulcers in a row on his right leg. The biopsy from the affected area was taken and cultured on Sabouraud's dextrose agar. What is the most likely causative organism?
A young child of 7 years of age is seen with indurated ulcers, lymphadenopathy and fever. The likely treatment is:
Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
Which of the following conditions is caused by Staphylococcus aureus?
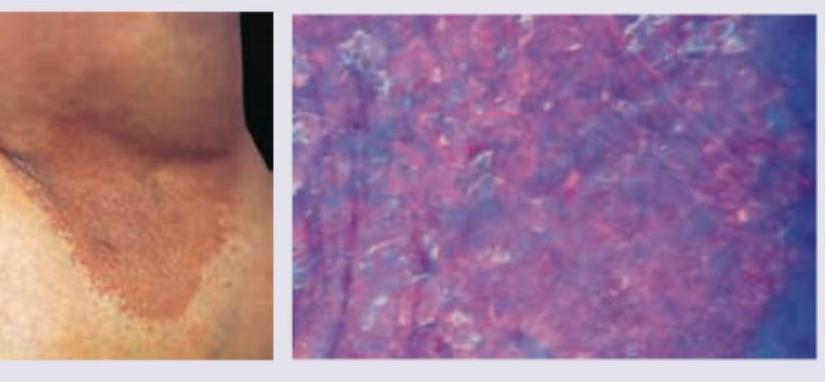
A 35-year-old obese woman presents with recurrent lesions in both axilla in summer season. Wood lamp examination is shown. The diagnosis is:
What is the treatment for granuloma inguinale?
A truck driver presents with a single painless genital ulcer that appeared 3 weeks after an unprotected sexual encounter. There is associated non-tender inguinal lymphadenopathy. What is the most likely diagnosis?
A patient presents with multiple painful genital ulcers associated with tender cervical/inguinal lymphadenopathy. The ulcers are soft and irregular as shown in the image. What is the most likely causative organism?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app