
Autoimmune Skin Diseases — MCQs

On this page
The following lesion appears on the cheek of a patient of ulcerative colitis. It subsided with potassium iodide treatment. What is the diagnosis?

The lesion shown below is seen in:

All are true about the lesions shown except:

All are true about the lesion shown below except:

All are true about the skin disease shown except:
A patient presents with the skin lesions shown in the image. While evaluating for possible blistering disorders, all of the following conditions could present with similar morphology EXCEPT:

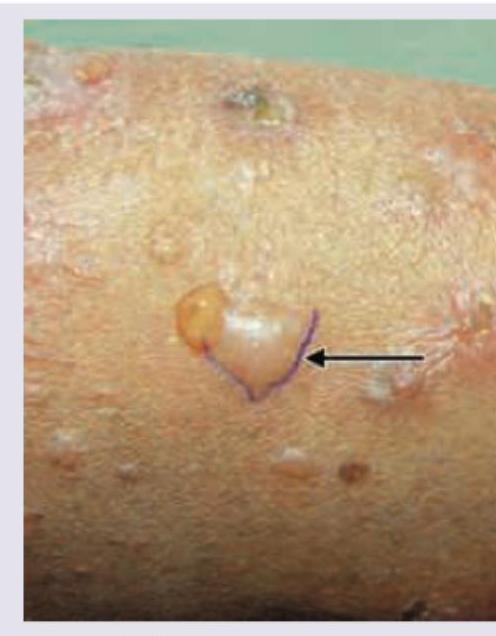
The following image shows a flaccid bulla with a positive Nikolsky sign. This finding is characteristically seen in:

The image shows:

Which of the following vesico-bullous disorders will exhibit the direct immunofluorescence shown below? (Recent NEET Pattern 2016-17)

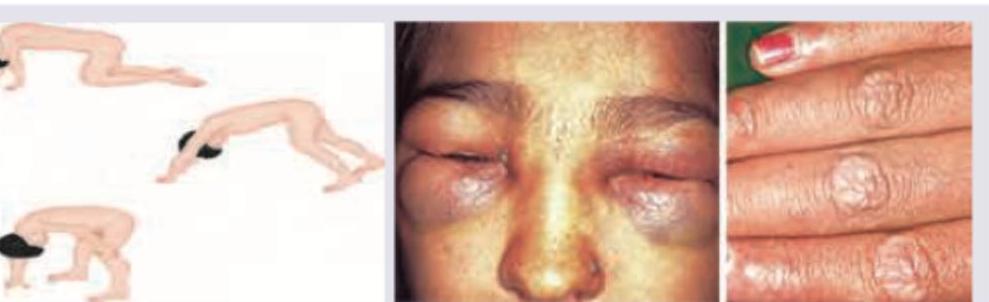
A 9-year-old girl presents with erythematous-to-violaceous papules over the extensor joints of the fingers and a heliotrope eruption over the upper eyelids. On physical examination following clinical sign was elicited. What is the most appropriate initial laboratory investigation?
Practice by Chapter
Lupus Erythematosus: Cutaneous Forms
Practice Questions
Lupus Erythematosus: Systemic with Skin Manifestations
Practice Questions
Dermatomyositis
Practice Questions
Scleroderma and Morphea
Practice Questions
Mixed Connective Tissue Disease
Practice Questions
Sjögren's Syndrome: Cutaneous Manifestations
Practice Questions
Relapsing Polychondritis
Practice Questions
Autoimmune Thyroid Disease and the Skin
Practice Questions
Immunobullous Disorders
Practice Questions
Vasculitis
Practice Questions
Diagnostic Methods in Autoimmune Dermatoses
Practice Questions
Management of Autoimmune Skin Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app