
Autoimmune Skin Diseases — MCQs

On this page
A patient presents with a photosensitive upper-back eruption on the upper back and shoulders (img-16.jpeg) and violaceous papules over the MCP and interphalangeal joints on hands (img-17.jpeg). What is the likely diagnosis?
A woman presents with pruritic rash on the elbows, buttocks with recent diagnosis of gluten sensitive enteropathy. On immunofluorescence IgA deposition is seen as shown in the image. What is the most likely diagnosis?
All the following statements regarding the image given are true except: (Recent Neet Pattem 2016-17)

What is the most likely diagnosis of the image given below?

A patient presents with violaceous papules over the knuckles and mottled pigmentation on the dorsum of hands. Identify the lesion:

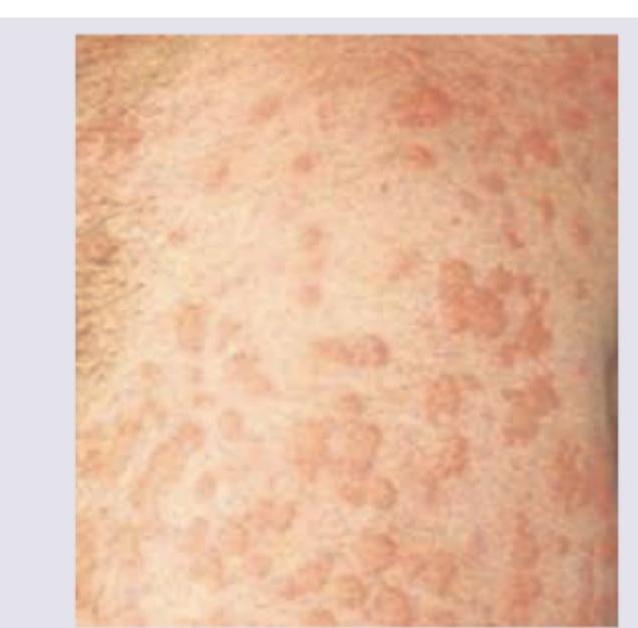
A 26-year-old female with a history of extensive exposure to sun comes to your clinic with presentation shown below. What is the most likely diagnosis?
Identify the lesion:

A patient presents with oral mucosal lesions. Identify the condition shown in the image:

An elderly patient presents with itchy tense blisters on normal looking skin as well as on urticarial plaques as shown below. The most probable diagnosis is: (AIIMS Nov 2015)

The following lesion appears on the leg of a patient of ulcerative colitis. All are useful in management except:

Practice by Chapter
Lupus Erythematosus: Cutaneous Forms
Practice Questions
Lupus Erythematosus: Systemic with Skin Manifestations
Practice Questions
Dermatomyositis
Practice Questions
Scleroderma and Morphea
Practice Questions
Mixed Connective Tissue Disease
Practice Questions
Sjögren's Syndrome: Cutaneous Manifestations
Practice Questions
Relapsing Polychondritis
Practice Questions
Autoimmune Thyroid Disease and the Skin
Practice Questions
Immunobullous Disorders
Practice Questions
Vasculitis
Practice Questions
Diagnostic Methods in Autoimmune Dermatoses
Practice Questions
Management of Autoimmune Skin Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app