
Autoimmune Skin Diseases — MCQs

On this page
A 28-year-old female presents with a 3-month history of violaceous, flat-topped papules on her wrists and lower back associated with intense pruritus. Examination reveals white lacy streaks on the buccal mucosa bilaterally. She was recently started on antihypertensive medication 4 months ago. Histopathology shows hyperkeratosis, irregular acanthosis, and band-like lymphocytic infiltrate at the dermoepidermal junction. What is the most appropriate next step in management?
A study of persons developing skin lesions following sun exposure is conducted. The lesions are not found on skin protected from ultraviolet light. Biopsies of involved skin show immunoglobulin G deposition along the dermal-epidermal junction, along with vacuolization of the basal layer and a perivascular lymphocytic infiltrate. No other organ involvement is present. Which of the following diseases do these patients most likely have?
Gottron's papules are a characteristic clinical finding in which of the following conditions?
Salt and pepper dyschromatosis is seen in which of the following conditions?
Which of the following drugs is not associated with drug-induced pemphigus?
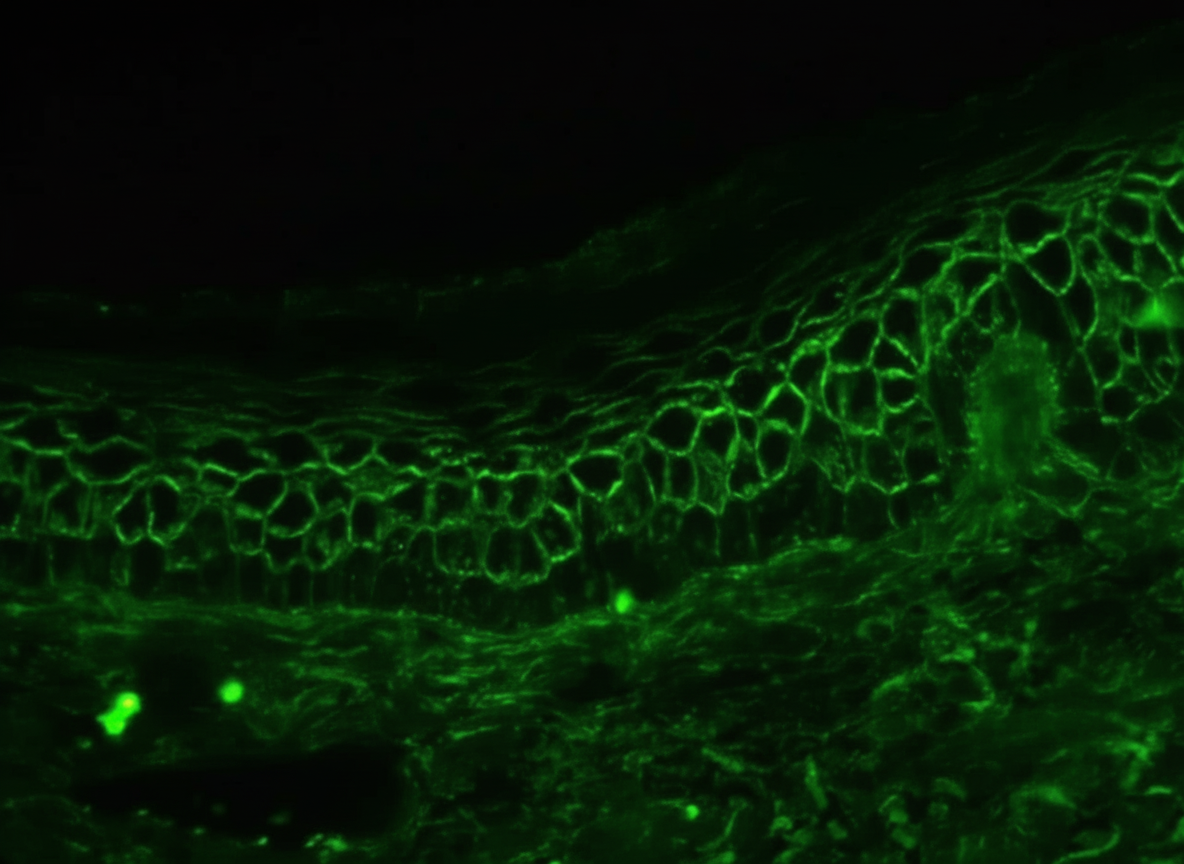
A 25-year-old man complains of eruptions of blisters on his scalp, inner surface of the groin, and in his mouth. The blisters rupture easily and leave large crusted areas. Histologically, the lesions show separation of the stratum spinosum from the basal layer. The results of direct immunofluorescence microscopy for IgG are shown. Which of the following proteins is targeted by IgG autoantibody in the skin of this patient?
Grinspan syndrome is associated with which of the following conditions?
Heliotrope sign is typically seen in which of the following conditions?
In pemphigus foliaceous, acantholysis is seen in which layer of the epidermis?
The Pathergy test is positive in which of the following conditions?
Practice by Chapter
Lupus Erythematosus: Cutaneous Forms
Practice Questions
Lupus Erythematosus: Systemic with Skin Manifestations
Practice Questions
Dermatomyositis
Practice Questions
Scleroderma and Morphea
Practice Questions
Mixed Connective Tissue Disease
Practice Questions
Sjögren's Syndrome: Cutaneous Manifestations
Practice Questions
Relapsing Polychondritis
Practice Questions
Autoimmune Thyroid Disease and the Skin
Practice Questions
Immunobullous Disorders
Practice Questions
Vasculitis
Practice Questions
Diagnostic Methods in Autoimmune Dermatoses
Practice Questions
Management of Autoimmune Skin Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app