
Public Health Administration — MCQs

On this page
Winslow's definition of public health does not include which one of the following concepts?
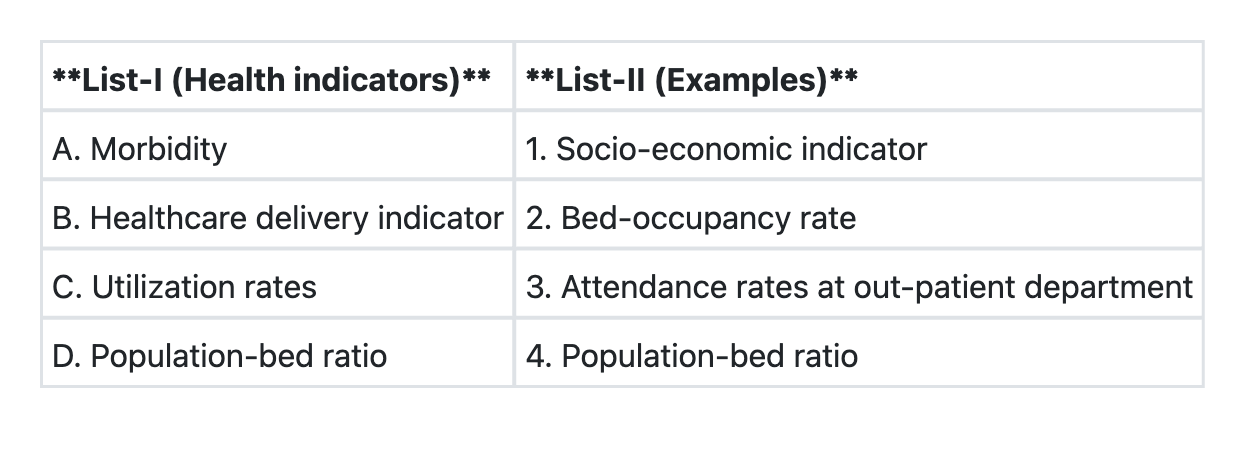
Match List-I with List-II and select the correct answer using the code given below the Lists: **List-I (Indicator Category)** A. Morbidity indicator B. Healthcare delivery indicator C. Utilization indicator D. Socio-economic indicator **List-II (Example)** 1. Literacy rate 2. Incidence rate of a disease 3. Bed-occupancy rate 4. Population-bed ratio
Health functionary at PHC level is:
Which among the following is/are the examples of primordial prevention ? 1. Adopting healthy lifestyles from childhood 2. Immunization of infants 3. Screening of cervical cancer Select the correct answer using the code given below:
The difference between Type A and Type B sub centre as per Indian Public Health standards is in terms of:
Which one of the following management techniques helps in standardising the methods of performing jobs ?
Consider the following staff: 1. Medical Officer 2. Pharmacist 3. Anaesthetist 4. Health Educator Of them, who are routinely posted to a PHC ?
Which of the following indicators stand consolidated in Physical Quality of Life Index (PQLI)? 1. Infant mortality 2. Life expectancy at age one 3. Per capita income 4. Literacy
Which one of the following is included in Indian Public Health Standards for a Primary Health Centre?
Consider the following: 1. Literacy rate 2. Life expectancy at birth 3. Life expectancy at the age of one year 4. Infant mortality Which of the above are the components of Physical Quality of Life Index (P.Q.L.I.)?
Practice by Chapter
Health Administration Structures
Practice Questions
National Health Programs
Practice Questions
District Health System
Practice Questions
Community Health Centers
Practice Questions
Primary Health Centers
Practice Questions
Sub-Centers
Practice Questions
Public Health Legislation
Practice Questions
Health Information Systems
Practice Questions
Health Management Information System
Practice Questions
Health Workforce Planning
Practice Questions
Public Health Ethics
Practice Questions
Intersectoral Coordination
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app