
Maternal and Child Health — MCQs

On this page
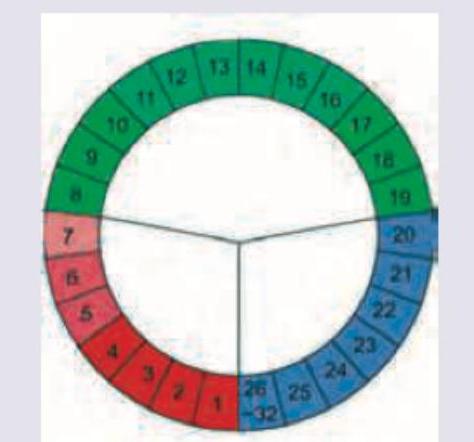
Identify the image given below:
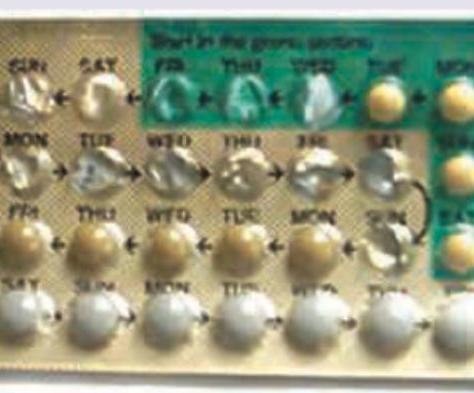
Identify the image given below:
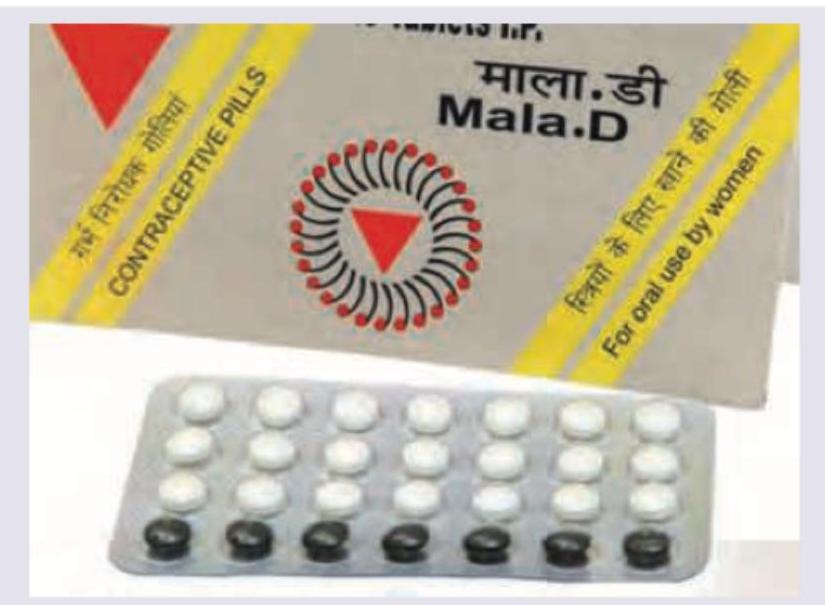
Select the correct composition of the OCP shown below:
Which is not correct regarding the contraceptive method being used?
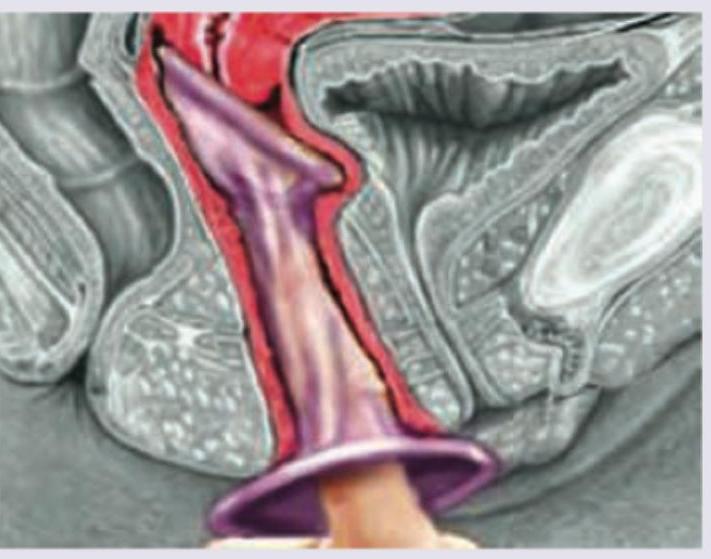
Identify the contraceptive method shown below:

Which programme provides an integrated package of supplementary nutrition, preschool non-formal education, immunization, health check-ups, referral services, and nutrition and health education for children and mothers?
Identify the program as given in the image:

The given image represents which of the following?

The logo represents which of the following?
The logo of which national health programme is shown below? (Recent NEET Pattern 2016-17)
Practice by Chapter
Maternal Mortality: Causes and Prevention
Practice Questions
Antenatal Care
Practice Questions
Intranatal Care
Practice Questions
Postnatal Care
Practice Questions
High-Risk Pregnancy Management
Practice Questions
Infant Mortality: Causes and Prevention
Practice Questions
Under-Five Mortality
Practice Questions
Integrated Management of Neonatal and Childhood Illness
Practice Questions
School Health Services
Practice Questions
Adolescent Health
Practice Questions
Reproductive and Child Health Programs
Practice Questions
International Maternal and Child Health Initiatives
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app