
Maternal and Child Health — MCQs

On this page
What is true about the New Born Care Corner (NBCC)?
What is the most common cause of death in children aged 1-4 years?
Salter's Scale is a useful method employed in the field to measure:
In a population of 1000, there are 200 eligible couples. 30 of them use condoms, 20 use IUCD, 20 use OC pills, while 70 have undergone female sterilization. The rest do not use any method. Calculate the Couple Protection Rate.
Which one of the following is a rare complication of the use of hormonal contraceptives?
In a community with a population of 10,000, there were 5 maternal deaths reported in the current year. If the birth rate is 36 per 1000, what is the Maternal Mortality Ratio (MMMR)?
What is the current neonatal mortality rate per 1000 live births?
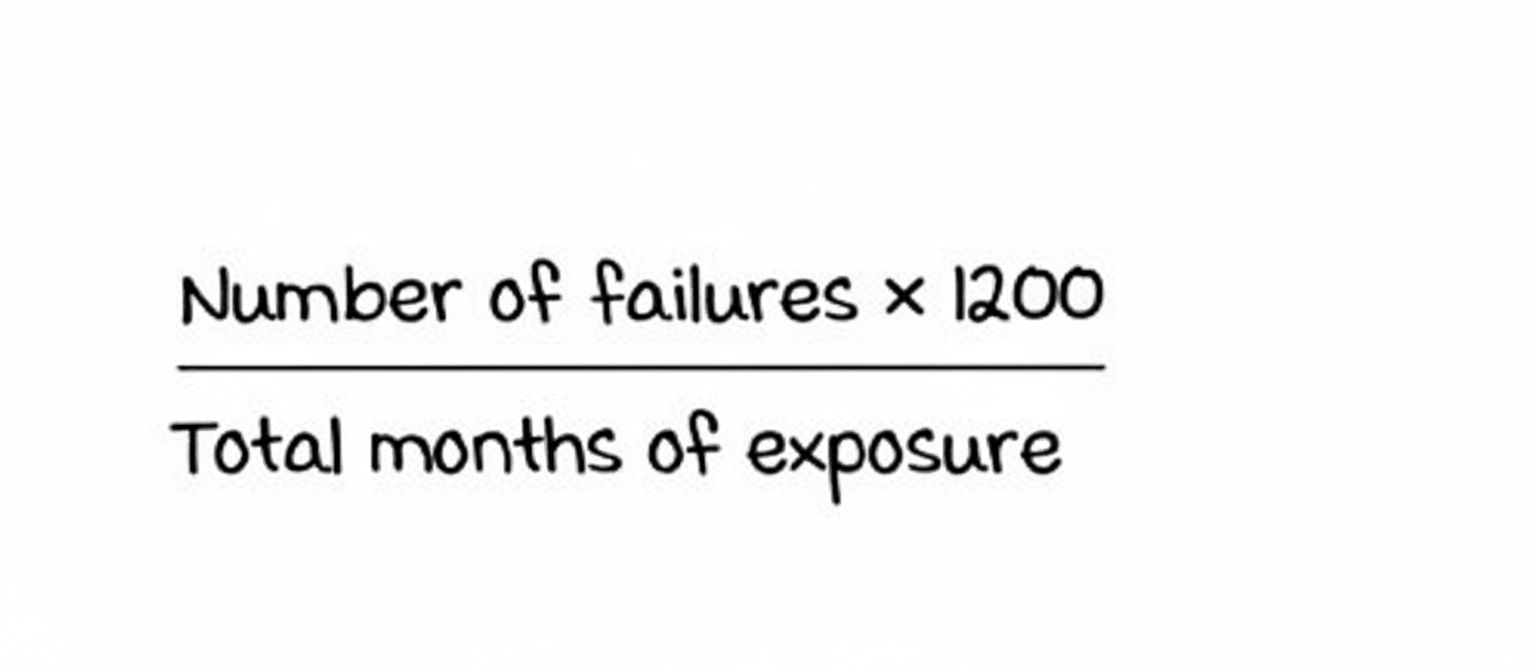
The formula shown is known as:
What is the Pearl Index of SAHELI?
What is the numerator in the maternal mortality ratio?
Practice by Chapter
Maternal Mortality: Causes and Prevention
Practice Questions
Antenatal Care
Practice Questions
Intranatal Care
Practice Questions
Postnatal Care
Practice Questions
High-Risk Pregnancy Management
Practice Questions
Infant Mortality: Causes and Prevention
Practice Questions
Under-Five Mortality
Practice Questions
Integrated Management of Neonatal and Childhood Illness
Practice Questions
School Health Services
Practice Questions
Adolescent Health
Practice Questions
Reproductive and Child Health Programs
Practice Questions
International Maternal and Child Health Initiatives
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app