
Biostatistics — MCQs

On this page
A physician, after examining a group of patients with a certain disease, classifies the condition of each one as 'Normal', 'Mild', 'Moderate', or 'Severe'. Which one of the following is the scale of measurement being adopted for classification of the disease condition?
What does the number of live births per number of females aged 15-45 in the population denote?
What is the denominator used for calculating the GFR (Glomerular Filtration Rate)?
What sampling method is used in assessing the immunization status of children under an immunization program?
Which of the following scales is used for quantitative data?
What is the median value for the following data set: 5, 5, 50, 150, 10, 20?
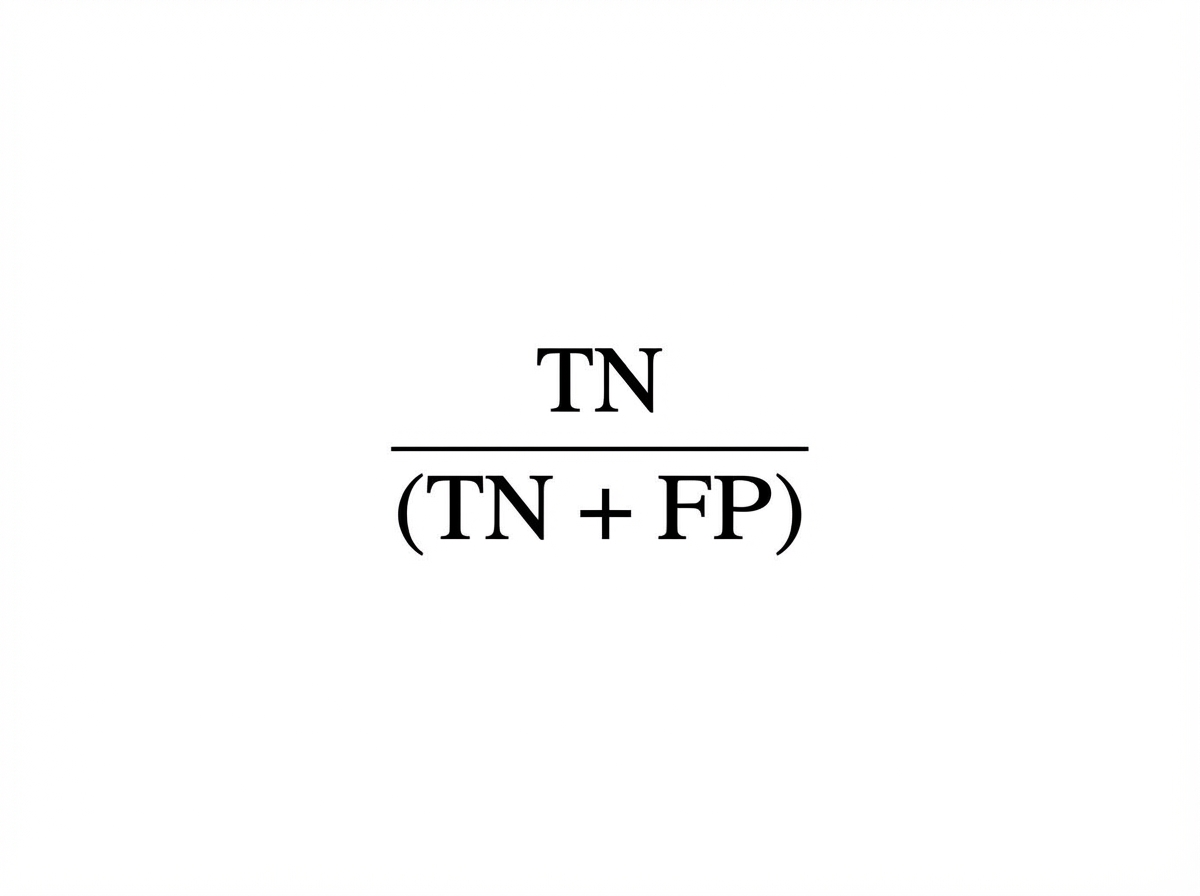
The formula denotes:
Which one of the following will be affected by inter-observer variation in epidemiological studies?
The male to female ratio is typically expressed as:
For the purpose of intervention trials, the preferred randomization unit is an individual for all of the following except?
Practice by Chapter
Collection and Presentation of Data
Practice Questions
Measures of Central Tendency
Practice Questions
Measures of Dispersion
Practice Questions
Normal Distribution
Practice Questions
Sampling Methods
Practice Questions
Sample Size Calculation
Practice Questions
Hypothesis Testing
Practice Questions
Tests of Significance
Practice Questions
Correlation and Regression
Practice Questions
Survival Analysis
Practice Questions
Multivariate Analysis
Practice Questions
Statistical Software in Research
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app