
Hemoglobin and Iron Metabolism — MCQs

On this page
Which of the following statements is true regarding the binding of O2 to hemoglobin?
Which of the following statements is NOT true regarding the buffering action of hemoglobin?
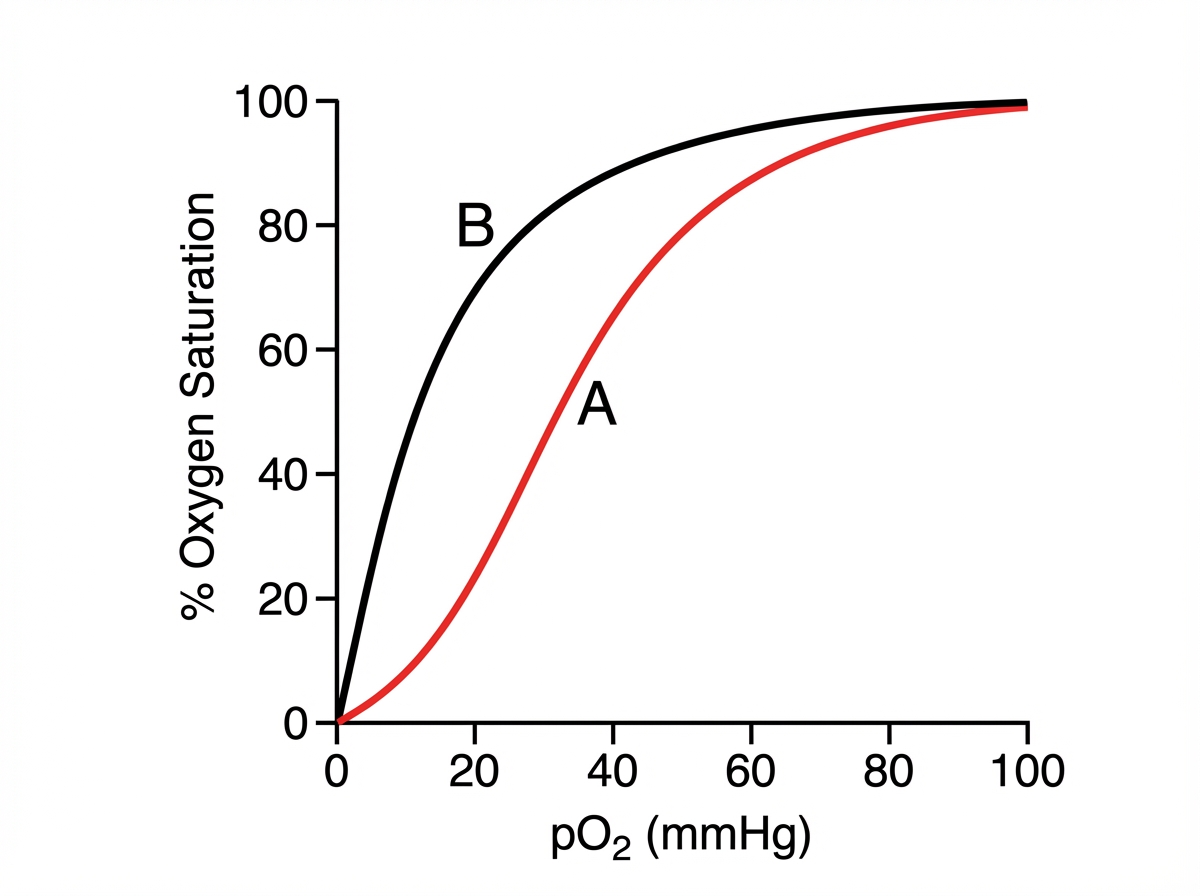
Study the given oxygen-hemoglobin dissociation curve and comment on the finding shown, identifying which protein corresponds to curve A and which to curve B.
A 10-year-old boy presented with muscle weakness and fatigue with increased lead in the blood. Which enzyme production in the liver is increased?
Hemoglobin electrophoresis in SC A (sickle cell anemia) shows the presence of which hemoglobin?
A missense gene mutation in the beta-globin chain is characteristic of which condition?
An Rh-negative woman delivered an Rh-positive infant. Within a few days after birth, the infant developed jaundice, ascites, hepatomegaly, and edema. What is the likely substance deposited in the skin and sclera in jaundice?
Iron in heme is linked to globin through which amino acid residue?
Pale lemon yellow color of urine is due to all except?
A patient presents with unconjugated hyperbilirubinemia and elevated urobilinogen levels in urine. What is the most likely diagnosis?
Practice by Chapter
Hemoglobin Structure and Function
Practice Questions
Oxygen Transport and Oxygen-Hemoglobin Dissociation Curve
Practice Questions
Hemoglobin Variants and Hemoglobinopathies
Practice Questions
Thalassemias
Practice Questions
Methemoglobin and Abnormal Hemoglobins
Practice Questions
Hemoglobin Synthesis
Practice Questions
Heme Synthesis and Porphyrias
Practice Questions
Iron Absorption and Transport
Practice Questions
Iron Storage and Recycling
Practice Questions
Disorders of Iron Metabolism
Practice Questions
Anemia: Biochemical Aspects
Practice Questions
Biochemistry of Hemostasis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app