
Genetic Disorders and Biochemical Pathology — MCQs

On this page
During evaluation of a child with intellectual disability following findings were noted. These point to deficiency of?
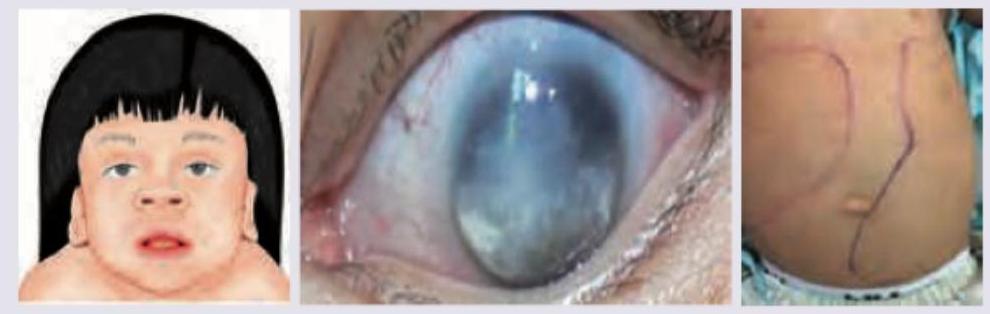
A 10-month-old child with coarse facies is referred for developmental delay. On examination, hepatosplenomegaly was noted. WBC N-acetylglucosamine-1-phosphotransferase activity was absent. The X-ray is shown below. What is the diagnosis?

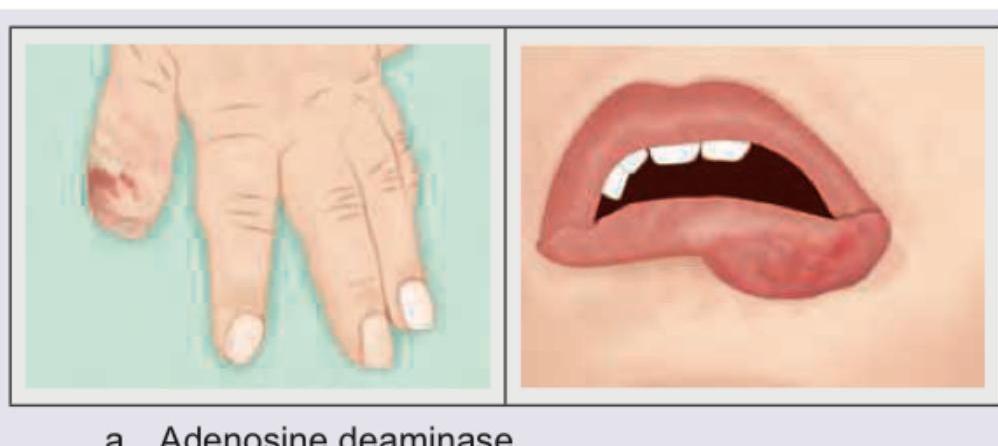
The patient shown here is suffering from deficiency of which enzyme?
The patient shown below has curly easily breakable hair. Which is correct about the condition?

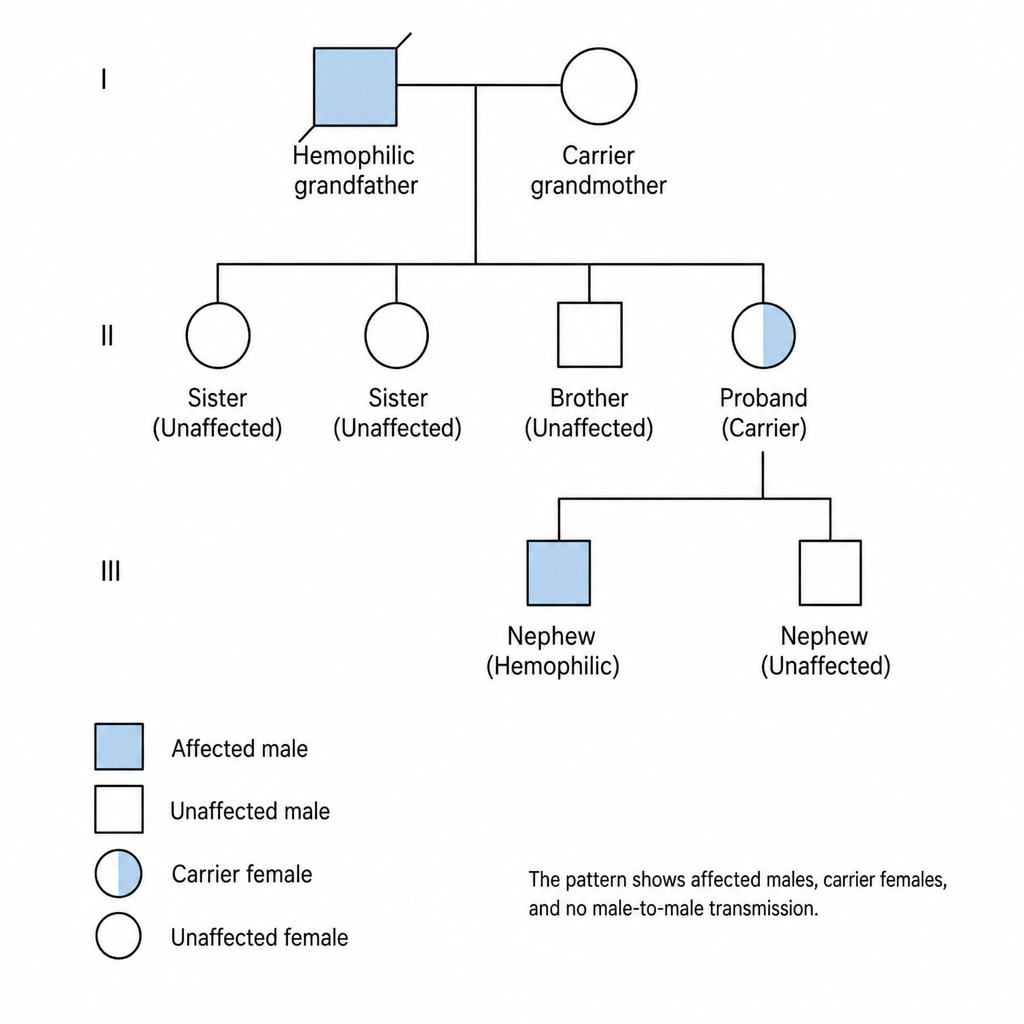
A 34-year-old, G1P0, presents for genetic counseling at 12 weeks' gestation. The patient has two sisters and a brother; her father has hemophilia. Her siblings are not affected, but she has a nephew that is afflicted. What is the inheritance pattern of this disorder? (Recent NEET Pattern 2016-17)
Wilson's disease has which of the following inheritance?
Which of the following is X-linked dominant trait?
Biochemical screening of newborn infants by heel-prick blood samples is performed by using the
Which one of the following conditions is NOT inborn error of metabolism?
Which membrane channel is mainly affected in Cystic fibrosis?
Practice by Chapter
Single Gene Disorders
Practice Questions
Biochemical Diagnosis of Genetic Disorders
Practice Questions
Inborn Errors of Metabolism
Practice Questions
Lysosomal Storage Diseases
Practice Questions
Glycogen Storage Diseases
Practice Questions
Disorders of Lipoprotein Metabolism
Practice Questions
Disorders of Purine and Pyrimidine Metabolism
Practice Questions
Hemoglobinopathies
Practice Questions
Porphyrias
Practice Questions
Biochemical Markers for Disease Diagnosis
Practice Questions
Newborn Screening for Genetic Disorders
Practice Questions
Enzyme Replacement Therapy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app