
Genetic Disorders and Biochemical Pathology — MCQs

On this page
Which of the following statements is FALSE regarding Crigler-Najjar syndrome type II?
Which genetic disease is exclusively transmitted to females?
Mitochondrial DNA linked disease is characterized by which mode of inheritance?
A one-month-old male infant presents with feeding difficulties and a history of frequent seizures. Blood investigations reveal elevated very long chain fatty acids (VLCFA). What is the likely diagnosis?
Which chromosome is involved in Angelman syndrome?
Which of the following genetic disorders does not have an available enzyme replacement therapy?
What is the inheritance pattern of congenital adrenal hyperplasia?
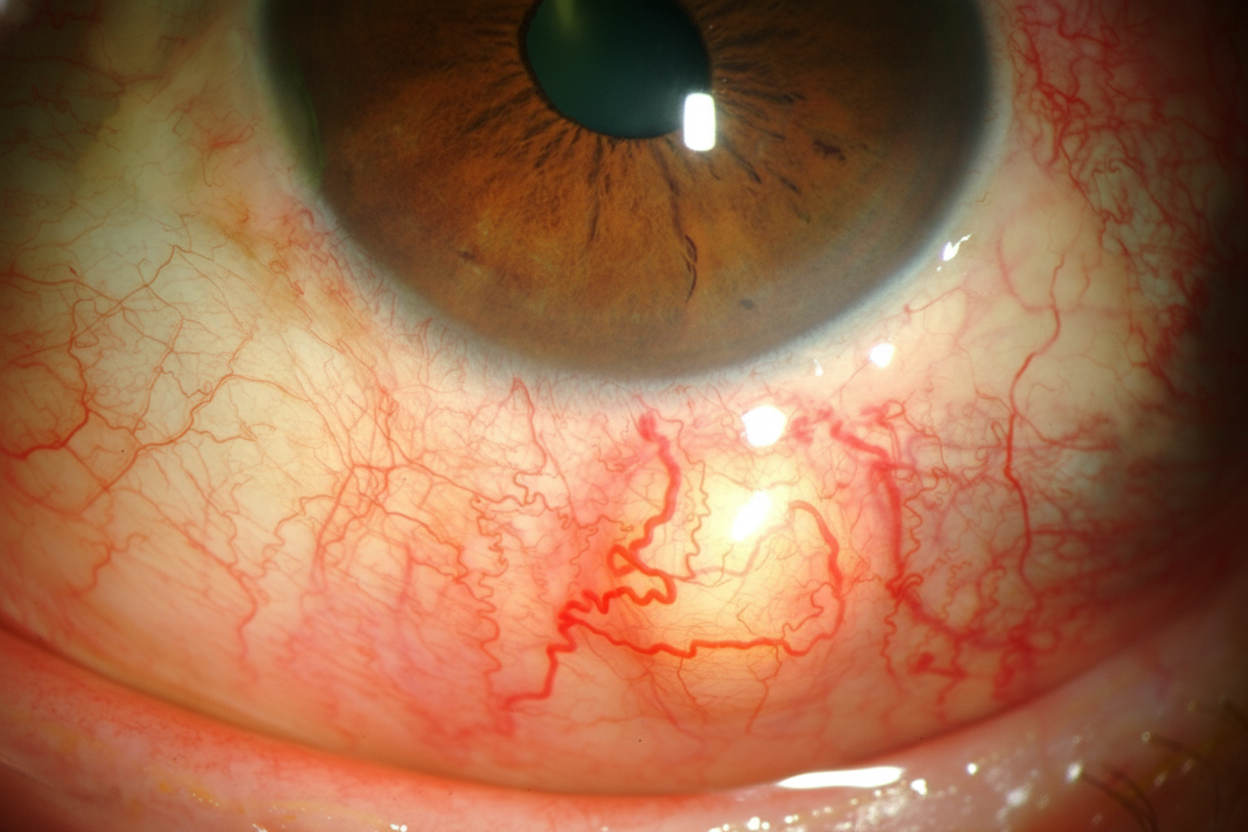
A child presents with progressive cerebellar ataxia, recurrent sinopulmonary infections, and the ocular finding shown in the image. The gene for this disease is localized to which chromosome?
A sick child presents with a low white blood cell count, metabolic acidosis, an increased anion gap, and mild hyperammonemia. Plasma amino acid measurements reveal elevated glycine, and urinary organic acid measurements reveal increased amounts of propionic acid and methyl citrate. Which of the following processes is most likely indicated?
Which of the following syndromes is/are associated with mitochondrial inheritance?
Practice by Chapter
Single Gene Disorders
Practice Questions
Biochemical Diagnosis of Genetic Disorders
Practice Questions
Inborn Errors of Metabolism
Practice Questions
Lysosomal Storage Diseases
Practice Questions
Glycogen Storage Diseases
Practice Questions
Disorders of Lipoprotein Metabolism
Practice Questions
Disorders of Purine and Pyrimidine Metabolism
Practice Questions
Hemoglobinopathies
Practice Questions
Porphyrias
Practice Questions
Biochemical Markers for Disease Diagnosis
Practice Questions
Newborn Screening for Genetic Disorders
Practice Questions
Enzyme Replacement Therapy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app