
Clinical Biochemistry — MCQs

On this page
A 10-year-old boy presents with increased bilirubin, bilirubin in urine, and no urobilinogen. What is the most likely diagnosis?
Which condition is characterized by hypocalcemia with hyperphosphatemia?
Cerebrospinal fluid (CSF) is best stored at which temperature?
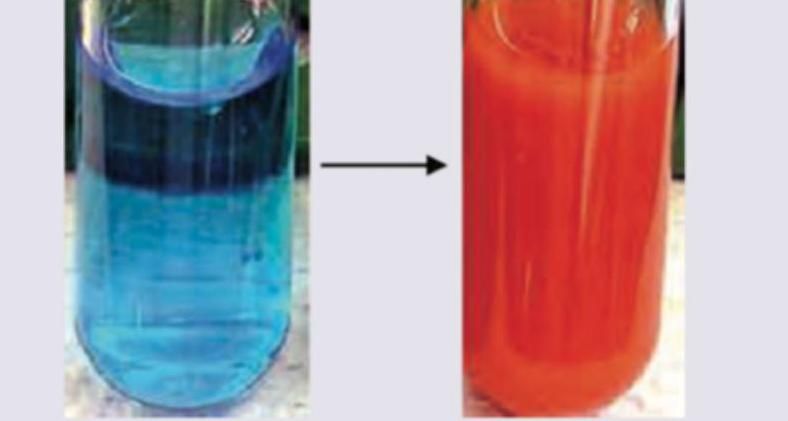
A 50-year-old male with family history for type 2 diabetes underwent a urine test for reducing substances. The test tube containing 0.5 ml of urine and 5 ml Benedict's reagent was put in a water bath for 2 minutes and a brick-red precipitate was observed. Which is the correct statement about the approximate concentration of reducing sugar in the urine sample?
A sample of 5 mL urine of the patient was taken and aqueous solution of picric acid was added to it. The solution was made alkaline using NaOH and the following colour was produced. The test is called?

Which of the following tubes contain sodium fluoride as an anti-coagulant?
Which one of the following conditions can be screened during neonatal screening by biochemical tests?
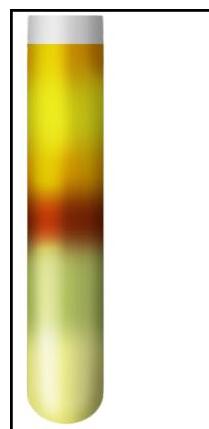
A urine sample shows a maroon-colored ring at the interface of two layers after adding reagents. Identify the test:
Preferred biochemical marker(s) in patients presenting with myocardial infarction:
In a child presenting with obstructive jaundice all are elevated EXCEPT:
Practice by Chapter
Liver Function Tests
Practice Questions
Kidney Function Tests
Practice Questions
Cardiac Markers and Enzymes
Practice Questions
Pancreatic Function Tests
Practice Questions
Glucose Tolerance Tests
Practice Questions
Lipid Profile and Cardiovascular Risk
Practice Questions
Tumor Markers
Practice Questions
Hormonal Assays and Interpretation
Practice Questions
Electrolytes and Acid-Base Balance Tests
Practice Questions
Cerebrospinal Fluid Analysis
Practice Questions
Point-of-Care Testing
Practice Questions
Quality Control in Clinical Biochemistry
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app