
Potassium Balance — MCQs

The body fluid compartments of a patient were measured, showing the following ion concentrations: - Sodium (Na): $10 \mathrm{mEq} / \mathrm{L}$ - Potassium (K): $140 \mathrm{mEq} / \mathrm{L}$ - Chloride (Cl): $15 \mathrm{mEq} / \mathrm{L}$ Based on these values, which fluid compartment is being described?
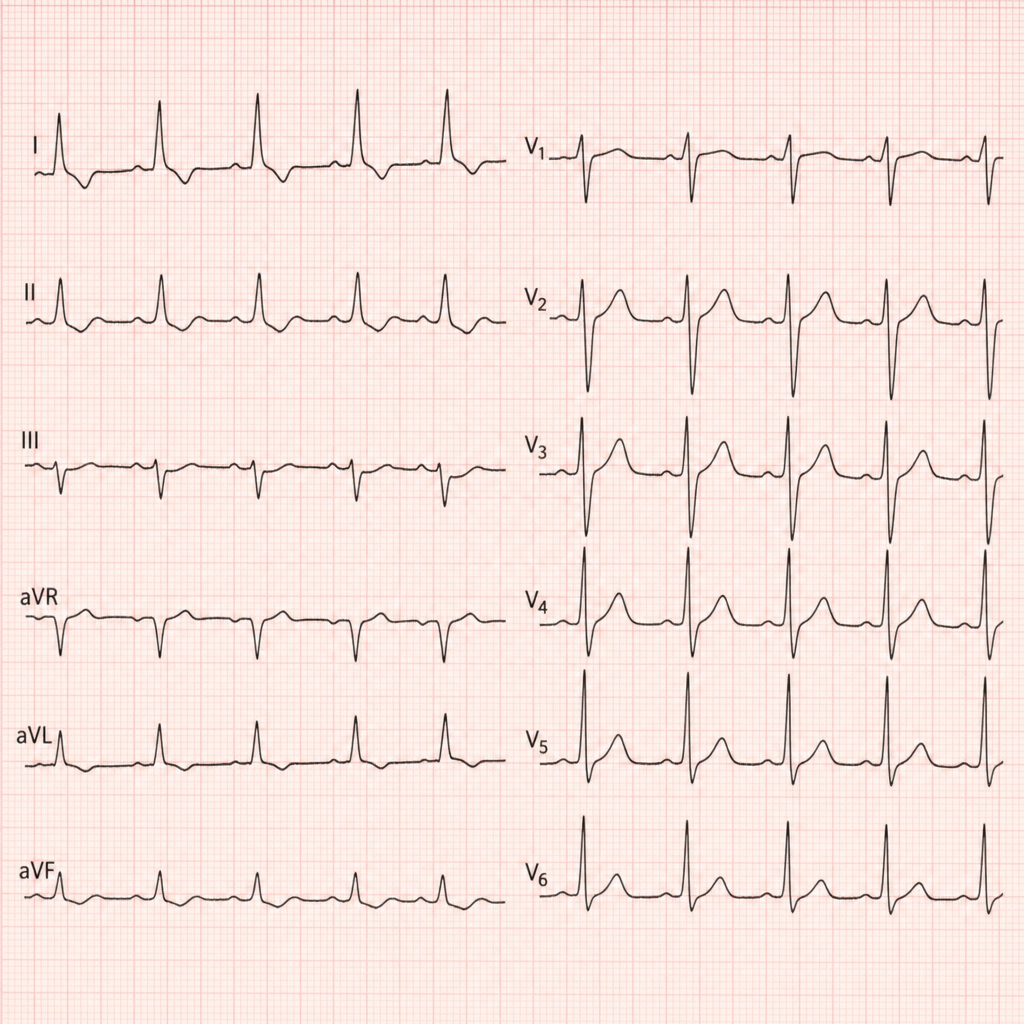
A patient with chronic kidney disease (CKD) presents with tachycardia, and the ECG is recorded as shown above. What is the most likely diagnosis?
Hypokalemia is seen in therapy with
All of the following are features of hyperkalemia on ECG, EXCEPT:
All of the following drugs are known to worsen hyperkalemia except
Hyperkalemia means more than
A patient has hyperaldosteronism. Which lab finding is expected?
Reduced osmolarity ORS does not contain which of the following ion?
Most clinically significant characteristic of Ringer's Lactate is -
Which of the following receptors mediate stretch reflex?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app