
Respiratory and Airway Management — MCQs

On this page
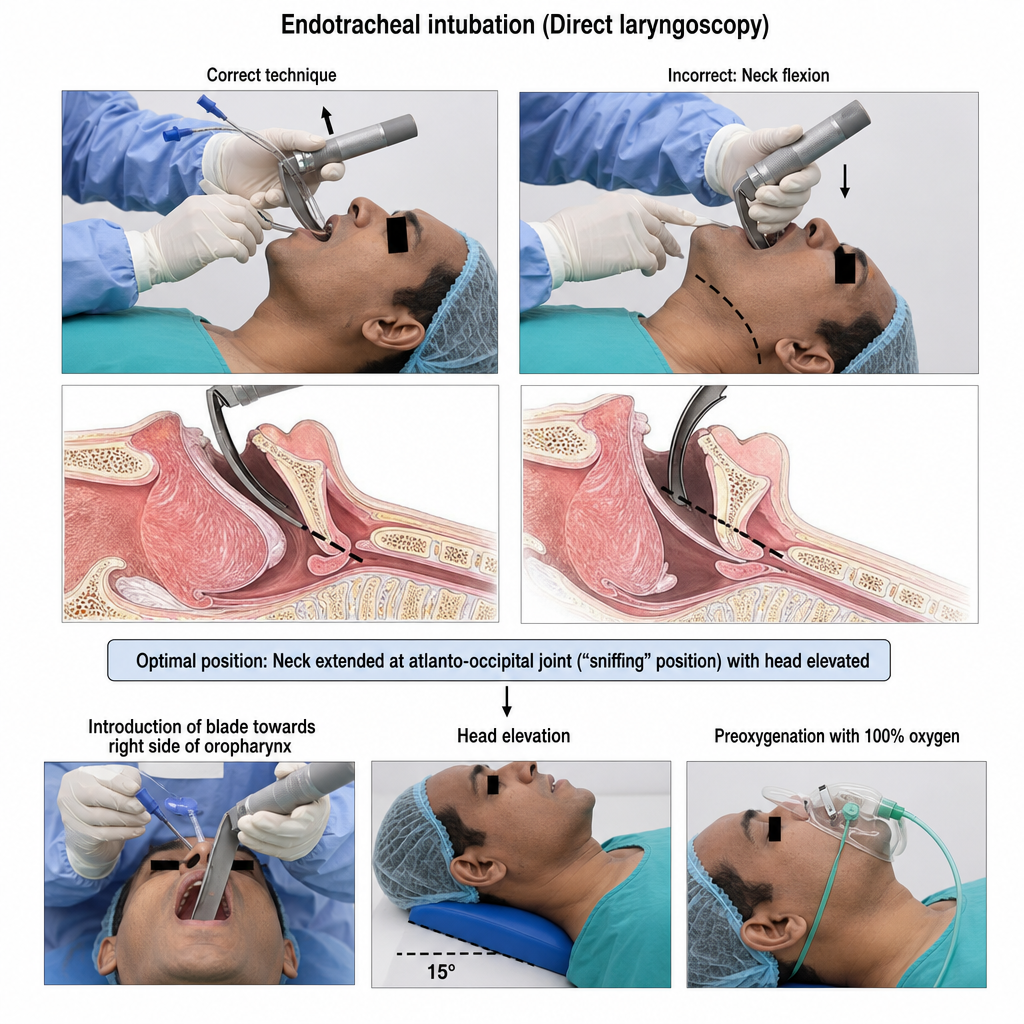
Which of the following is NOT true about endotracheal intubation?
Which of the following is a fixed oxygen delivery device?
Which of the following ventilation modes reduces work of breathing by overcoming the resistance created by ventilator tubing?
Which of the following conditions are contraindications for both oral and nasal intubation?
A Macintosh curved blade laryngoscope is a type of:
Which of the following is contraindicated during this procedure?
What is a contraindication for nasotracheal intubation?
What is the best method for airway maintenance in a patient experiencing cardiopulmonary arrest?
What is the Bailey maneuver in patients at high risk of laryngospasm?
What is the best indicator of successful endotracheal tube extubation?
Practice by Chapter
Respiratory Physiology
Practice Questions
Airway Anatomy
Practice Questions
Preoxygenation Techniques
Practice Questions
Mask Ventilation
Practice Questions
Supraglottic Airway Devices
Practice Questions
Direct Laryngoscopy
Practice Questions
Video Laryngoscopy
Practice Questions
Fiberoptic Intubation
Practice Questions
Surgical Airway Management
Practice Questions
One-Lung Ventilation Techniques
Practice Questions
Ventilation Strategies During Anesthesia
Practice Questions
Extubation Criteria and Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app