
Respiratory and Airway Management — MCQs

On this page
What complication is NOT seen with controlled ventilation?
Which of the following is NOT a step in rapid sequence intubation?
Identify the pictured airway device.

In a young patient with extensive soft tissue and muscle injury, which muscle relaxant used for endotracheal intubation might lead to cardiac arrest?
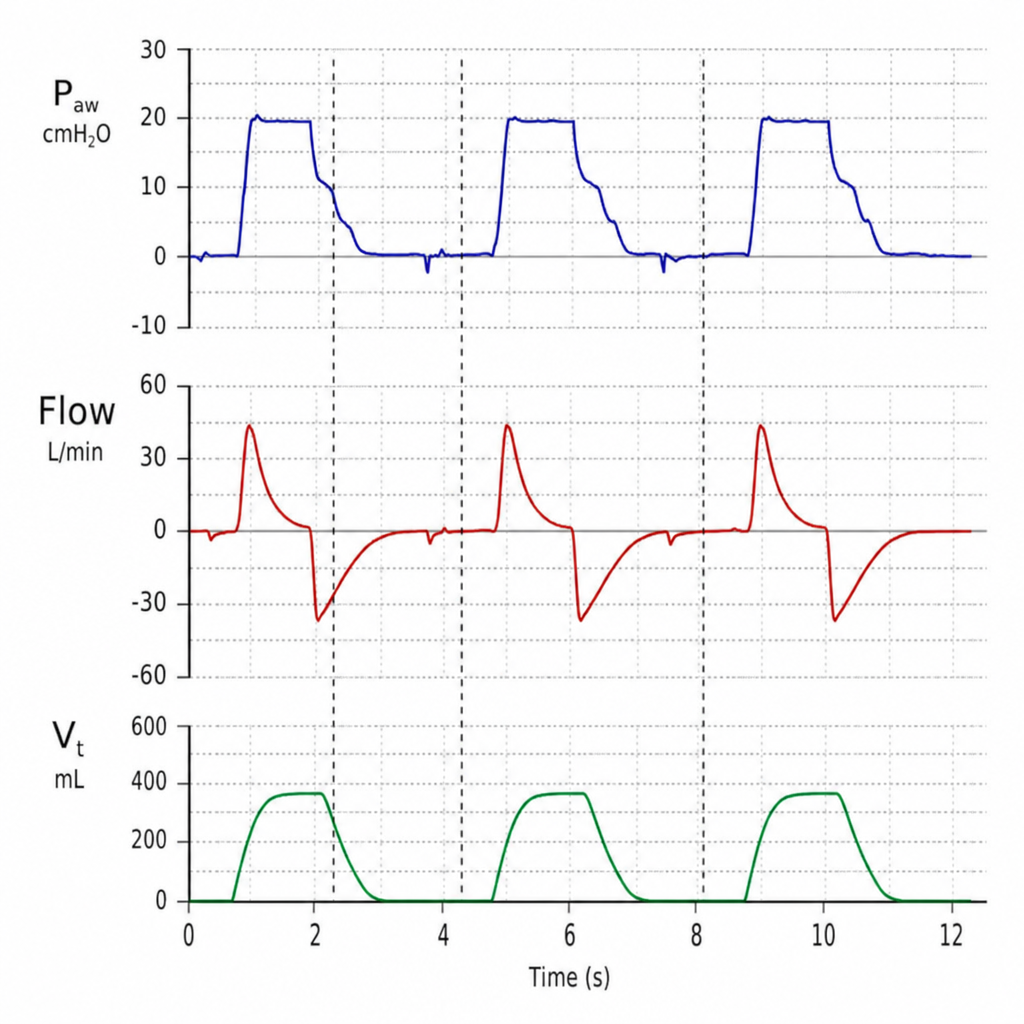
The ventilation chart shown depicts:
During a preoperative assessment of the airway, only the hard palate is visible when the patient phonates. What is the grade according to the modified Mallampati test?
Generally accepted indications for mechanical ventilatory support include which of the following?
What are the pulmonary changes in the lateral position in an anesthetized patient?
What is the method to establish a safer airway in a patient with neck trauma and cricoid fracture, with a possibility of a difficult airway?
A 6-year-old patient, admitted for a dog bite on the face, developed anaphylaxis to a test dose of Augmentin, presenting with stridor requiring immediate intubation. As the sole physician available, and with a No. 3 curved blade laryngoscope ready, what is the appropriate internal diameter of the endotracheal tube to request?
Practice by Chapter
Respiratory Physiology
Practice Questions
Airway Anatomy
Practice Questions
Preoxygenation Techniques
Practice Questions
Mask Ventilation
Practice Questions
Supraglottic Airway Devices
Practice Questions
Direct Laryngoscopy
Practice Questions
Video Laryngoscopy
Practice Questions
Fiberoptic Intubation
Practice Questions
Surgical Airway Management
Practice Questions
One-Lung Ventilation Techniques
Practice Questions
Ventilation Strategies During Anesthesia
Practice Questions
Extubation Criteria and Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app