
Respiratory and Airway Management — MCQs

On this page
Preoperative Samsoon and Young modified, Mallampati test is used for assessing:
Rapid Sequence Induction is indicated in:
A patient is found unresponsive. On assessment, the patient has a detectable pulse but absent normal breathing. What is the appropriate interpretation of this clinical finding?

In which clinical scenario would you find a patient requiring the resuscitation technique shown in the image?

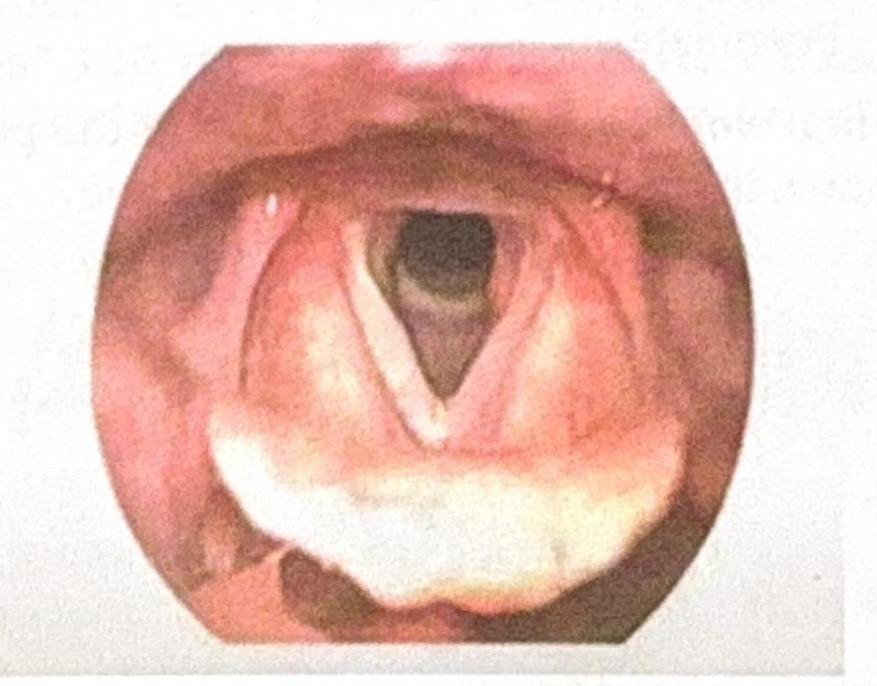
The image shows the glottic view obtained during laryngoscopy for intubation. Which classification system is used to grade this laryngeal view?
What is the purpose of Positive End-Expiratory Pressure (PEEP)?
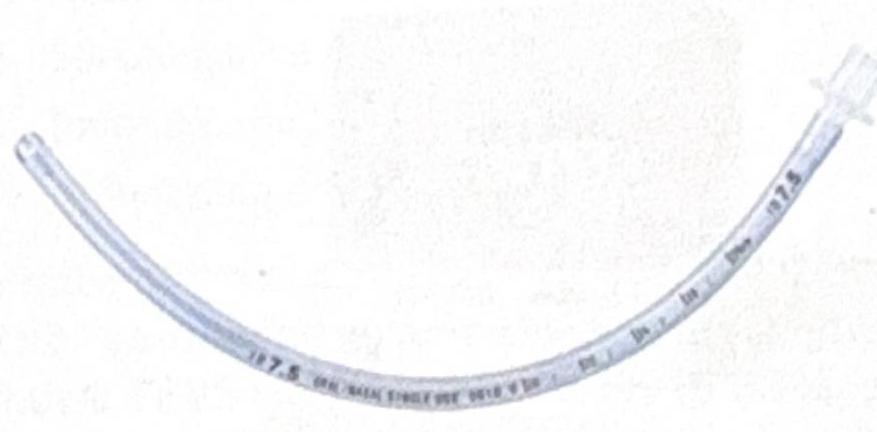
Identify the instrument shown in the image:
The procedure shown in the image is performed to maintain the airway. Which of the following techniques is being used?

In conventional oxygen therapy, which device will deliver the highest FiO2?
Endotracheal tube in the esophagus is best assessed by:
Practice by Chapter
Respiratory Physiology
Practice Questions
Airway Anatomy
Practice Questions
Preoxygenation Techniques
Practice Questions
Mask Ventilation
Practice Questions
Supraglottic Airway Devices
Practice Questions
Direct Laryngoscopy
Practice Questions
Video Laryngoscopy
Practice Questions
Fiberoptic Intubation
Practice Questions
Surgical Airway Management
Practice Questions
One-Lung Ventilation Techniques
Practice Questions
Ventilation Strategies During Anesthesia
Practice Questions
Extubation Criteria and Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app